
Occupational Blood Lead Surveillance Of Construction Workers, II -Health Programs in Thirteen States
Summary Statement
A study reviewing the adult blood lead surveillance system used in each of 13 states, with an emphasis on construction workers
1997
Abbreviations
| ABLES | Adult Blood Lead Epidemiology and Surveillance |
| DOT | Department of Transportation (state level) |
| NIOSH | National Institute for Occupational Safety and Health |
| OSHA | Occupational Safety and Health Administration |
| SIC | Standard Industrial Classification |
| µg/dl | Micrograms per deciliter |
Survey Methods
General Findings
- Trends in Surveillance
- Reporting and Intervention Practices
- Blood Lead Levels
- Lead-in-Construction Initiatives
Recommendations
- Increased Funding
- Targeted Education Efforts
- Uniform Data Collection
- Interagency Cooperation
Tables
- Surveyed states, 1996 and 1995
- Adult blood lead surveillance in 13 states, 1996
- Surveyed states' construction worker population, bridge repair funds, and number of deficient bridges, circa 1994
Alabama
Alaska
Florida
Idaho
Indiana
Kentucky
Mississippi
North Carolina
Oregon
Pennsylvania
South Carolina
Tennessee
West Virginia
Annex
B. Questionnaire Sent to States
Annex
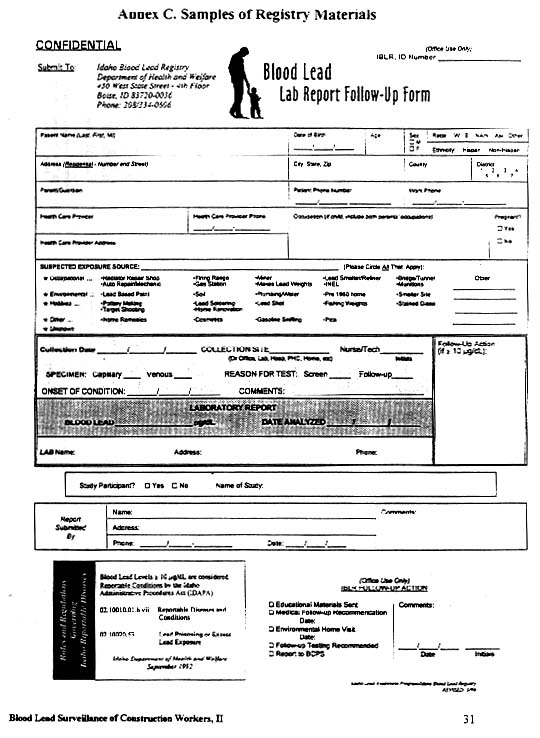
C. Samples of Registry Materials
Annex
D. State Agency Contacts
In 1995, researchers at the Irving J. Selikoff-Mount Sinai Center for Occupational and Environmental Medicine and at the New York State Department of Health, Division of Occupational and Environmental Epidemiology, surveyed 12 state departments of health. The results of that survey were published in November 1995 by CPWR – Center for Construction Research and Training as Occupational Blood Lead Surveillance of Construction Workers: Health Programs in Twelve States.
In 1996, the authors continued to survey state health agencies; the results of the survey of 13 additional states are reported here. Both surveys were designed to examine (1) trends in lead surveillance activities, both general and construction-specific; (2) the degree to which cooperative efforts have emerged among state agencies to address construction workers' lead exposures; and (3) perceived barriers to program development and implementation.
According to the National Institute for Occupational Safety and Health (NIOSH), 95% of reported adult blood lead levels result from occupational lead exposure. Home repair and hobbies also contribute to adult lead exposure. In the late 1980s and early 1990s, reports of lead poisoning among construction workers began to rise (National Institute for Occupational Safety and Health 1992). In 1993, the U.S. Occupational Safety and Health Administration (OSHA) promulgated the Lead Exposure in Construction standard (Occupational Safety and Health Administration 1993).
Lead-based paint has been applied to virtually all steel bridges, elevated highways and railways, and storage tanks in the United States. Construction workers employed in rehabilitation or demolition of steel structures -- bridges and storage tanks -- face an elevated risk of lead exposure and concomitant health effects. Painters, laborers, and ironworkers are particularly at risk on these projects. With infrastructure repair on the rise, the number of workers and the extent of their exposures to lead are likely to increase.
In 1990, the US Public Health Service issued Healthy People 2000, announcing a national health objective to eliminate all lead exposures that result in blood lead levels greater than 25 micrograms per deciliter (µg/dl) (Public Health Service 1990). OSHA's Lead Exposure in Construction standard in 1993 set a blood lead level of 40 µg/dl as the trigger for intervention at a worksite. However, a recent epidemiological study of elderly men with long-term environmental exposure to lead indicated that lower blood lead concentrations may cause health effects, such as impaired renal function (Kim and others 1996). (The definition of an "elevated" blood lead level varies among states.)
Although a handful of states began developing surveillance systems for adult lead poisoning as early as the 1970s, most states established such registries in the 1980s and 1990s. In most cases, states have set up adult blood lead registries following or in conjunction with the establishment of childhood lead poisoning surveillance and prevention programs. NIOSH's Adult Blood Lead Epidemiology and Surveillance (ABLES) program has been a major force in support of states' efforts to establish adult registries. ABLES provides funding and technical support to states to document and prevent adult lead poisoning in high-risk industries and occupations, including construction. NIOSH publishes ABLES states' combined reports of adult blood lead levels each quarter in the Center for Disease Control and Prevention's publication, Morbidity and Mortality Weekly Report.
Registries are created through state legislation or agency administrative procedures, such as amendments to a reportable disease rule. These laws and rules mandate the reporting of blood lead levels to a specific state agency, usually the department of health. Adult blood lead registries generally rely on laboratories, physicians, and/or other health care entities such as clinics and hospitals to report elevated blood lead levels.
A registry's foremost function is surveillance. Registry surveillance activities can include collecting, analyzing, and reporting data in order to examine the distribution of adult lead poisoning. Categories analyzed may include occupation, industry sector, geographic location, and time period. The detection of trends can be useful for determining program priorities for prevention and research initiatives and for evaluating the effectiveness of intervention strategies. Some information needed for this surveillance work is available on a state's blood lead-level reporting form. Most often, however, registry staff must conduct extensive report follow-up to obtain basic information on the characteristics of the individual and the circumstances of the exposure.
In addition to surveillance, some registries intervene to prevent or reduce lead poisoning. Intervention typically includes giving information to lead-poisoned people about the health hazards of lead, methods to control exposures, and appropriate medical care. A registry may also provide information to physicians and/or employers, depending on the registry's intervention protocol. In some instances, an industrial hygiene investigation will occur, or a case will be referred to state or federal OSHA for a follow-up investigation. Some registries have undertaken broad-based public health initiatives such as conferences on occupational lead exposure and targeted mass mailings of educational materials. In addition, as documented in the previous study, some registries have undertaken special programs to prevent lead poisoning of construction workers.
The states in the current survey were selected based on geographic diversity (table 1). The survey questionnaire covered registry background information, reporting requirements, data-collection and response protocols, and any special surveillance programs in construction (see annexes A and B). The questionnaire used in the 1995 survey was revised for this effort, in order to improve clarity.
As with the first survey, the survey was faxed to an identified contact person in each state and an appointment was made to complete the survey by telephone interview. Interviews took place during the summer. Registry personnel then reviewed their state's summary and changes were made to the summaries accordingly.
Trends in Surveillance
The survey found
that 10 of 13 states require the reporting of adult blood lead levels.
Indiana, Mississippi, and West Virginia do not have adult blood lead registries.
| Table 1. Surveyed states, 1996 and 1995 | ||||||
| 1996 (Current report) | 1995 (Previous report) | |||||
| Alabama | California | |||||
| Alaska | Connecticut | |||||
| Florida | Georgia | |||||
| Idaho | Louisiana | |||||
| Indiana | Maryland | |||||
| Kentucky | Massachusetts | |||||
| Mississippi | Michigan | |||||
| North Carolina | New Jersey | |||||
| Oregon | New York | |||||
| Pennsylvania | Ohio | |||||
| South Carolina | Texas | |||||
| Tennessee | Washington | |||||
| West Virginia | ||||||
Seven of the 10 states implemented reporting requirements for adult blood lead levels in the 1990s. Kentucky, Pennsylvania, and South Carolina have required the reporting of adult blood lead levels since the early 1970s.
NIOSH's ABLES program helps fund registry operations in five states: Alabama, North Carolina, Oregon, Pennsylvania, and South Carolina.
Reporting and Intervention Practices
In the 10 states with blood lead registries:
- Laboratories are required to report blood lead test results (table 2). Physicians are also required to report test results in all of the states except Pennsylvania.
- Blood lead levels triggering reporting range from all test results (South Carolina) to 40 µg/dl (North Carolina). Six of the states require reporting at 15 µg/dl or higher: Alabama, Alaska, Florida, Idaho, Pennsylvania, and Tennessee. In Pennsylvania, the 15 µg/dl threshold applies only to pregnant women; for others the threshold is 25 µg/dl.
- Four states --Alabama, Idaho, North Carolina, and Oregon -- have mechanisms to identify a person's occupation, usually through case follow-up. Alabama and Oregon maintain statistics on occupational versus non-occupational cases. Only Oregon has systematically classified whether occupational cases belong to the construction sector or general industry.
- Seven registries undertake intervention efforts in addition to data collection. The most common intervention activity is providing educational materials on lead's health effects and exposure prevention. Intervention activities also include telephone follow-up with physicians and/or with individuals having elevated blood lead levels.
- Of the seven states that intervene, four have set intervention-triggering levels at 25 µg/dl or greater.
- Six states refer cases of elevated blood lead levels to the state or federal OSHA for investigation.
- No registry conducts industrial hygiene worksite investigations or intervention. The North Carolina Department of Health has industrial hygienists on staff and is developing procedures for deploying them in worksite investigations of elevated blood lead-level cases. Alabama and Oregon also plan to conduct such investigations.
Blood Lead Levels
As with our first survey, the survey found that insufficient and noncomparable data made year-to-year and interstate trends impossible to elucidate. Only six states provided data for both 1993 and 1994. Three of those states showed an increase the number of cases or reports. (A report is counted each time an individual takes a test and cases represent an individual's highest blood lead level report for a given year.) One state showed a decrease and two states had too-few reports to chart a change. Interstate comparisons were further complicated by the range in categorization. For example, several states reported their highest category as 60 µg/dl and above, while Oregon's highest category was 40 µg/dl and above.
In 1993-94, reports in the highest category collected (60 µg/dl or greater) in Pennsylvania declined from 2.8% to 0.9% of the total. In South Carolina, although the total number of cases increased dramatically, the number of cases at 60 µg/dl or greater decreased from 5.0% to 2.0% of the total.
Only Oregon had data available on blood lead level by employment sector. Oregon's 1994 data show that 6 of the 49 cases (12%) of blood lead levels 40 µg/dl or greater were from the construction sector. North Carolina had data on cases by employment sector, but not by blood lead level. In 1994, North Carolina registry staff found that 4 of 244 reported cases (1.6%) were from the construction sector.
Lead-in-Construction Initiatives
North Carolina, Pennsylvania, and South Carolina have initiated some construction-focused activities. These activities include attempts at interagency cooperation with the North Carolina and Pennsylvania Departments of Transportation and conferences on lead health issues targeting the construction industry in Pennsylvania and South Carolina (annex C). The South Carolina conference was held in 1994, although the state does not currently have construction-focused activities. Registry staff in Idaho reported that special surveillance of blood lead levels in the construction sector is under consideration.
| Table 2. Adult blood lead surveillance in 13 states, 1996 | ||||||
| State | Registry?a | Who reports to the stateb | Reporting
threshold (µg/dl) |
Action taken? | Level (µg/dl) triggering state action |
Construction-
focused activities? |
| Alabama | Y (1991) | L, P, O | 15 | N | N | N |
| Alaska | Y (1996) | L, P, O | 10 | Y | To be decided | N |
| Florida | Y (1992) | L, P, O | 10 | N | N | N |
| Idaho | Y (1992) | L, P, O | 10 | Y | 10 | U |
| Indiana | N | -- | -- | -- | -- | -- |
| Kentucky | Y (1974) | L, P, O | 25 | N | N | N |
| Mississippi | N | -- | -- | -- | -- | -- |
| North Carolina | Y (1993) | L, P | 40c | Y | 25 | Y |
| Oregon | Y (1991) | L, P | 25 | Y | 25 | N |
| Pennsylvania | Y (1975) | L | 25; 15 for pregnant women | Y | 60 | Y |
| South Carolina | Y (1971) | L, P, O | All | Y | 40 | N |
| Tennessee | Y (1995) | L, P | 10 | Y | Case by case | N |
| West Virginia | N | -- | -- | -- | -- | -- |
|
||||||
Registry staff have sought to implement the following activities to address lead poisoning prevention in construction: interagency-sponsored conferences aimed at contractors, union representatives, and health care providers; review of DOT construction specifications; joint department of health-DOT inspections of worksites, department of health review of blood lead level results for DOT projects; and ongoing communication between registry staff and DOT and department of labor staff.
Among the 13 states surveyed in 1996, Pennsylvania, North Carolina, and Tennessee ranked first through third, respectively, in terms of numbers of construction workers, deficient bridges, and bridge repair dollars (table 3). Registry staff in Pennsylvania and North Carolina are aware of the special lead hazard to construction workers and have initiated efforts to work with their DOTs to address the problem.
| Table 3. Surveyed states' construction worker population, bridge repair funds, and number of deficient bridges, circa 1994 | |||
| Number of
construction workersa |
Bridge repair
funds ($ millions) b |
Number of deficient bridgesc | |
| Alabama | 81,600 | $36.1 | 5,201 |
| Alaska | 12,100 | $6.4 | 212 |
| Florida | 298,300 | $45.3 | 2,628 |
| Idaho | 29,000 | $6.4 | 790 |
| Indiana | 127,500 | $35.3 | 5,112 |
| Kentucky | 74,000 | $33.8 | 4,571 |
| Mississippi | 44,200 | $41.0 | 6,580 |
| North Carolina | 165,000 | $64.9 | 6,006 |
| Oregon | 61,600 | $35.8 | 1,789 |
| Pennsylvania | 202,800 | $257.1 | 9,771 |
| South Carolina | 84,300 | $27.4 | 1,884 |
| Tennessee | 101,200 | $60.7 | 5,456 |
| West Virginia | 34,100 | $54.4 | 3,023 |
| Total | 1,315,700 | $704.4 | 53,023 |
| Average | 101,208 | $54.2 | 4,079 |
|
|||
- As in the first survey, the researchers found that registries are underfunded, understaffed, and overextended. Very often, staff have multiple responsibilities in addition to lead surveillance, including surveillance of other mandated reportable conditions such as infectious diseases. In addition, data collection problems are compounded by a lack of compliance by reporting entities (such as, laboratories), forms that omit important information, and limited resources to perform necessary follow-up.
- Despite this lack of staff and funding, seven (70%) of the registries surveyed had intervention components in addition to data collection activities. However, these efforts were generally not case-specific and were limited to the provision of educational information to physicians and individuals having elevated blood lead levels. Some registry staff reported that they lacked a legal mandate to intervene in workplaces to prevent lead exposures. Others said it was not their role to intervene, that it was more appropriate for physicians or department of labor staff to contact employers about workplace conditions.
- While registry personnel in some states have had success in working with Dots, many still find that Dots are somewhat reluctant to embrace department of health initiatives to address the lead hazard in construction. Barriers to interagency cooperation include the fact that public health has traditionally been outside the mission of Dots, a difference in language and working styles between the public health and engineering professions, and budgetary constraints that dictate different priorities in two agencies. Even within their own health agencies, some registry staff did not feel that there was support for construction-focused activities.
- None of the states surveyed had yet successfully implemented a comprehensive preventive program in the construction sector. Beyond the lack of resources to undertake such efforts, other barriers included a lack of awareness of the problem of lead exposure in the construction trades among health department personnel. Those registries that had made efforts to reach out to state Dots reported that they often found limited support for prevention activities from transportation agencies.
- The sparseness of the data provided by the registries does not permit conclusions about the patterns and distribution of blood lead levels in adults. The figures reported are most likely an underestimate of the number of workers with elevated blood lead levels. While this conclusion may apply to workers in all sectors, there is reason to believe that construction workers are especially underrepresented in registry data. Given the level of infrastructure repair underway, the fact that 90% of bridges are coated with lead-based paints, and the substantial number of workers currently involved in infrastructure repainting and repair projects, the low number of reports suggests that construction workers are not being tested or their tests are not being reported to state registries.
Because registries can play an important role in preventing occupational blood lead poisoning, their surveillance and intervention activities should be funded at higher levels. NIOSH support and development funding through the ABLES program should be directed toward the expansion of state programs and the establishment of registries in states that do not yet have them. Additionally, state government resources should be sought.
Targeted Education Efforts
NIOSH should continue and intensify its efforts to educate state health and transportation departments about the special hazards and exposure issues related to lead in construction, specifically targeting states receiving substantial bridge repair funding. On the state level, health departments should review available data on the construction sector, such as numbers of deficient bridges and construction workers in their states. ("Deficient" is defined in table 3, note c.) These data can be useful, not only to educate health department personnel about the extent of construction activities in their states, but also to target intervention activities.
Uniform Data Collection
As states establish or revise their registry requirements, they should adopt the following policies:
- All adult blood lead test results should be reported, regardless of level.
- The occupation, industry sector, and employer of the patient should be reported with blood lead level results.
- Registries should assign Standard Industrial Classification (SIC) codes to cases, in order to identify trends, target intervention efforts, and standardize categories for analysis.
To facilitate national tracking and state-to-state comparisons with the limited resources presently available, the Centers for Disease Control and Prevention (CDC) and NIOSH should intensify efforts to develop a uniform data collection system.
Interagency Cooperation
Health agencies should initiate interagency cooperation among state and local health, labor, and transportation agencies to develop joint programs aimed at protecting workers from lead exposure. Building and construction trade unions should be called on to participate in such efforts. In particular, health agencies should advocate for the adoption of DOT project specifications designed to protect construction workers from lead (See CPWR – Center for Construction Research and Training 1993, for model specifications produced by a coalition representing government, the private sector, public interest groups, and universities).References
CPWR – Center for Construction Research and Training. 1993. Model Specifications for the Protection of Workers from Lead on Steel Structures. Washington, DC, Report OSH 3-93.
Federal Highway Administration, Department of Transportation. 1995. The Status of the Nation's Highway Bridges. Washington, DC: US Government Printing Office, June.
Kim, Rokhokim, Andrea Rotnitzky, David Sparrow, Scott Weiss, Carrie Wager, and Howard Hu. 1996. A Longitudinal Study of Low-level Lead Exposure and Impairment of Renal Function, Journal of the American Medical Association, 275 (15): 1177-81, April.
National Institute for Occupational Safety and Health, Department of Health and Human Services. 1992. NIOSH Alert: Request for Assistance in Preventing Lead Poisoning in Construction Workers. Cincinnati, Ohio: Centers for Disease Control, April.
Occupational Safety and Health Administration. 1993. Lead Exposure in Construction; Interim Final Rule. 29 CFR Part 1926. Federal Register 58 (84): 26590-26649, May 4.
Public Health Service, Department of Health and Human Services. 1990. Healthy People 2000: National Health Promotion and Disease Objectives. Washington, DC: DHHS Pub. No. (PHS) 91-50212.
Annex A. State Summaries
In 1991, lead was added to the list of more than 50 reportable diseases in Alabama. (State agency contacts are listed in annex D.) Physicians, dentists, nurses, medical examiners, hospital administrators, nursing home administrators, laboratory directors, school principals, and day care center directors are required to report blood lead levels of 15 µ/dl or greater for adults and children. Out-of-state laboratories are not required to report, although some do. On the whole, registry staff say, blood lead level reporting is low because of a lack of enforcement. The registry is concentrating on improving laboratories' compliance with reporting requirements and on setting up a more effective database.
In 1993 and 1994, the registry had funding from the National Institute for Occupational Safety and Health's Adult Blood Lead Epidemiology and Surveillance (ABLES) program, which supported 50% of a staff epidemiologist. This funding was discontinued in 1995, but was reinstated in September 1996. Currently, only 2% of the registry staff time is dedicated to adult blood lead surveillance, with the balance of efforts focused on communicable diseases.
Blood Lead Levels
In 1993, the registry received reports of 1,089 cases with blood lead levels 15 µg/dl or greater. (Information on the levels of these cases was not available.) Occupational information was provided for 35% (380) of these cases. Only one of these cases was construction-related.
In 1994, 1,036 cases were reported. Occupation was reported for 76% (784) of these cases, with 18% (140) of the cases for which occupation was identified having blood lead levels greater than 40 µg/dl. No cases were identified from the construction sector.
Follow-up Protocol
Currently, there is no follow-up protocol or intervention action, because of limited staff and resources. Blood lead level reports are filed for future entry into an improved database. The registry director occasionally conducts an informal investigation by phone, if he is concerned about a report. Plans for the ABLES funding include contracting for industrial hygiene services to conduct site investigations and provide consultations to companies whose workers have elevated blood lead level reports.
Referrals to OSHA
Referrals to federal OSHA are made case by case. The registry has referred only two cases in recent years.
Construction Initiatives
There are no special initiatives in construction, nor are any under consideration. Alabama has 5,201 deficient bridges (see table 3, note c), received $36.1 million in bridge repair funds in 1994, and had an average of 81,600 construction workers that year.
Alaska established its adult blood lead registry in January 1996. Laboratories and health care professionals, including doctors, nurses, hospitals, and village health aides, are required to report blood lead levels equal to or greater than 10 µg/dl within four weeks of a blood test. Information on a tested individual's occupation may be available if the tests are carried out in an occupational setting. Otherwise, information is obtained through case follow-up.
Blood Lead Levels
Because the registry was only established in January 1996, data are not yet available. However, in the late 1980s and early 1990s, the Alaska Department of Health conducted blood lead screenings of adults and children in a handful of mining areas. Although several hundred workers, residents, and children were tested in these screenings, very few elevated levels (greater than or equal to 10 µg/dl) were found in any group.
Follow-up Protocol
The registry is currently developing follow-up procedures and has not yet hired a registry administrator. Cases of elevated occupationally related levels identified prior to the establishment of the registry were dealt with on a case-by-case basis. If the Department of Health received a call from an individual or his or her physician regarding an elevated level, information was obtained on possible sources of exposure. Department of Health staff generally intervened to prevent exposure and followed cases until the situation was resolved. The staff do not include industrial hygienists, however The Department of Health has worked with industrial hygienists from the Department of Labor.
Referrals to OSHA
Cases are not referred to OSHA.
Construction Initiatives
The registry did
not anticipate any special initiatives in construction. With its one highway
and only 212 "deficient" bridges --as defined by the US Federal Highway
Administration (table 3) -- Compared with an average
of more than 4,000 deficient bridges per state in our survey, Alaska may
rank as a low-risk state for exposures to lead during construction. Alaska
tied Idaho for receiving the lowest amount of federal bridge repair funds
in 1994 ($6.4 million) among the 13 surveyed states. There are 12,100
construction workers (seasonally adjusted average) in Alaska. Registry
staff felt that construction would not be contributing many elevated blood
lead cases to the registry due to the newness of buildings and structures
and the short construction season. Most occupational lead exposure has
been observed in the mining and ore-processing sectors.
Lead poisoning, defined as a blood lead level of 10 µg/dl or greater in adults or children, became a reportable disease in Florida in 1992. Physicians, laboratories, other health professionals, and anyone else who comes into possession of a blood lead level test result of 10 µg/dl or greater is required to report it to a county public health unit or the state Health and Rehabilitative Services, State Health Office (the Department of Health equivalent for Florida), which then reports blood lead levels (of adults or children) to the Childhood Lead Poisoning Surveillance Program. There is no surveillance system specifically for adults. Reports received from the state's public laboratory -- a minority of reports received -- include complete information on a tested individual's name, address, birth date, and test result. This information allows the registry to distinguish adults' from children's reports. No information on occupation is collected. Reports from private laboratories, which perform most adult blood lead sample analyses, vary in their completeness.
Blood Lead Levels
Public laboratories submitted 16 adult reports in 1993 and 11 in 1994. However, registry staff suspect that these figures underestimate the extent of blood lead poisoning in the state, because most adult blood lead tests are analyzed by private laboratories.
Follow-up Protocol
The registry does not generally receive information that would allow it to determine if reports are for adults or are occupationally related. However, in instances where the registry or a county public health unit receives a report of 40 µg/dl or greater, and the identity and occupation of a case is known, the agency will report the case to the Florida Department of Labor, if the individual is a public employee, or to OSHA. County public health units have consulted with the registry about case follow-up.
Referrals to OSHA
As mentioned above, it is Florida's policy for the registry and county public health units to report cases of 40 µg/dl or greater to the Florida Department of Labor, if the individual is a public employee, or to OSHA.
Construction Initiatives
There are no special construction initiatives under way or planned in Florida. Florida has more construction workers (298,300) than any other state in this survey. In 1994, Florida received $45.3 million in bridge rehabilitation funds for its 2,628 bridges (see table 3, note c).
Idaho
In September 1992, the Idaho Department of Health and Welfare issued a regulation requiring health care providers, local health departments, and laboratories to report all blood lead levels of 10 µg/dl or higher for both adults and children. Adults are defined as individuals over age 17. Out-of-state laboratories are also required to report blood lead levels of Idaho residents. Registry personnel use the registry to prevent both adult and children's lead poisoning. However, except for the Panhandle, a major mining and smelting area in Idaho, children's lead exposure is thought to be minimal and adult occupational lead exposure is the focus of prevention efforts.
Blood Lead Levels
In 1993, the first year of the registry, only 11 cases were reported to the registry. In 1994 this figure went down to 8. The low level of reporting was attributed to the newness of the requirement. Of reported cases, registry staff estimated that 95% were occupationally related. To date, there have been no reported cases from the construction sector. Although there were too few cases to elucidate trends in 1993-94, it is interesting to note the pattern similar to other states. From 1993 to 1994, there was a decrease in higher-level cases and an increase in lower-level cases, with an overall decrease in total cases.
Follow-up Protocol
To date, follow-up has been attempted for all reports over 10 µg/dl. As reports become more numerous, a threshold for action is likely to be established. In all cases, registry staff send follow-up forms to the health care provider or the person who ordered the test in order to solicit information, such as the occupation of the individual tested and the specific source of the exposure (see annex C). Notice of the elevated report is also given to the state epidemiologist and the local health district. Registry personnel generally defer to the physician who ordered the test to handle the case. Registry staff have observed that physicians are lax in returning follow-up forms and are generally not well prepared to intervene on their patient's behalf to prevent occupational lead exposure. However, if the physician or the individual requests assistance, registry or health district staff can provide information and environmental assessment services. In one case, the registry initiated contact with the industrial hygienist of a gunpowder factory, following the receipt of an elevated report. In all cases, registry intervention is by request only.
Referrals to OSHA
Cases are not referred to OSHA.
Construction Initiatives
The registry has not received any reports to date from the construction sector. However, registry staff reported that, as a result of this survey, they intend to start tracking construction-related cases. Idaho has few deficient bridges relative to other states in this survey -- 790 compared to an average of more than 4,000 bridges per state surveyed (see table 3, note c). Idaho, along with Alaska, received the least amount of federal bridge repair funds in this group of states ($6.4 million) in 1994. There is a seasonally adjusted average of 29,000 construction workers in Idaho.
| Adult blood lead cases, Idaho, 1993 and 1994 | ||||
| Blood lead level (µg/dl) | 1993 Total cases | 1994 Total cases | ||
| Less than 25 | 4 | 6 | ||
| 25-39 | 5 | 2 | ||
| 40-59 | 1 | 0 | ||
| 60-79 | 0 | 0 | ||
| 80+ | 1 | 0 | ||
| Total | 11 | 8 | ||
Adult blood lead levels are not currently a reportable condition in Indiana. Staff of the Department of Health's Epidemiology Resource Center have been involved in researching and organizing a registry for Indiana since 1994. Policy discussions regarding revisions to the "reportable conditions rule" have included amendments to add adult blood lead levels. However, due to budgetary considerations, resource center staff were not hopeful about the prospects for an adult blood lead registry. According to Department of Health staff, Indiana is home to several lead industries and has a higher relative proportion of lead-exposed workers than most states. Additionally, Indiana has 5,112 bridges (surveyed states averaged 4,000 deficient bridges per state; see table 3), received $35.3 million in federal bridge money in 1994, and has an average of 127,500 construction workers.
Kentucky
Lead poisoning was made a reportable disease in Kentucky in 1974. Physicians, hospitals, clinical laboratories, and employers are required to report adult blood lead levels of 25 µg/dl or greater to the Kentucky Elevated Lead Level Registry. Out-of-state laboratories are required to report blood lead levels and are subject to financial penalties for noncompliance. The registry receives many out-of-state laboratory reports, especially from the large, national labs.
Blood Lead Levels
Registry staff estimate that they receive several hundred adult blood lead level reports per year and that most of the blood lead levels are between 25 and 40 µg/dl. Most laboratory reports do not include age or occupation. Reports from employers are the only source of occupational information. A database for blood lead levels was established in 1990, but due to limited resources, the database is not maintained.
Follow-up Protocol
When the database was first established, blood lead levels of 10 µg/dl or greater were entered into it. Currently, staff file the hard copies of reports. No follow-up is done.
Referrals to OSHA
Cases are not referred to Kentucky OSHA.
Construction Initiatives
Although a state statute regarding lead abatement activities took effect in July 1996, the registry does not anticipate any special surveillance initiatives in construction. As of 1994, Kentucky had 4,571 deficient bridges and received $33.8 million in federal bridge repair funding (see table 3, note c). The state has 74,000 construction workers (seasonally adjusted average).
Mississippi has no adult blood lead surveillance requirement or program. Some adult blood lead levels are reported to the state Childhood Blood Lead Registry, but those records are not maintained nor monitored. If Department of Health personnel conduct an environmental assessment as a result of an elevated level in a child, and find that a parent's "take-home" lead is the source of the child's exposure, the department provides information to the worker on controlling his or her exposure.
Mississippi has 6,580 bridges deemed deficient by the Federal Highway Administration, the second highest number in our survey. In 1994, the state received $41.0 million in bridge repair funds and has a seasonally-adjusted average of 44,200 construction workers.
Occupational Blood Lead Registry
In 1993 North Carolina enacted an occupational illness reporting requirement that included elevated adult blood lead levels. The law took effect January 1, 1994 and requires that laboratories report adult blood lead levels of 40 µg/dl or greater. Physicians are required to report elevated blood lead levels if the analysis is conducted by an out-of-state laboratory that fails to report a test for the physician's patient. The registry has requested that laboratories voluntarily report all blood lead levels of 25 µg/dl or greater, and has generally received cooperation with this request. The registry is located in the Occupational and Environmental Epidemiology Section of the Department of Environment, Health and Natural Resources.
Blood Lead Levels
In 1994, its first year, the registry catalogued 224 cases of individuals whose blood lead levels were 25 µg/dl or greater. In 1995, 342 cases were reported. The rise in the number of cases from 1994 to 1995 was attributed to increased reporting from smaller and out-of-state laboratories. In 1994, 68% of the cases were related to lead-acid battery manufacture or handling; 2% (4 cases) were related to construction; in 19%, occupationally related status was unknown; and the remaining 11% were from other industries or not occupationally related. Construction blood lead level reports were between 30 and 40 µg/dl. The highest levels reported to the registry were not related to an individual's occupation, but a hobby -- home manufacture or drinking of moonshine whiskey. (Homemade stills use vehicle radiators, containing lead solder.)
Follow-up Protocol
Following the receipt of a blood lead level greater than 25 µg/dl, the registry solicits complete information on the individual, including his or her employer and occupation, by a letter to the laboratory client, usually a physician. The individual with the elevated blood lead level is then sent a brochure on occupational lead poisoning. Registry staff are currently developing new educational materials: one for individuals with elevated blood lead levels, one for employers on their responsibilities under OSHA, and one for physicians on their reporting responsibilities. In rare cases of very high levels, phone interviews are conducted to determine the cause of the elevated lead level. Staff are also developing new procedures to determine when telephone interviews should be conducted; when cases should be referred to the Division of Occupational Safety and Health, in the state Department of Labor; and when inspections should be carried out by industrial hygienist staff from the registry.
Referrals to OSHA
The Department of Environment, Health and Natural Resources signed a Memorandum of Agreement with the Division of Occupational Safety and Health in February 1995. The agreement states that the registry can make referrals to the Division of Occupational Safety and Health for worksite investigations and must notify the agency if registry staff plan to conduct a worksite investigation themselves.
Construction Initiatives
As of yet there are no special initiatives to track blood lead levels among construction workers. However, the registry has approached DOT about a intervention project that would include medical surveillance. The registry is interested in pursuing the project in the future if funding is available. Additionally, legislation is pending at the state level for the certification and training of lead abatement workers.
North Carolina ranks second-highest in bridge repair money ($64.9 million in 1994) among the states surveyed here. There are 6,006 deficient bridges in North Carolina, compared to the surveyed states' average of 4,000, and 165,000 construction workers -- more on average than in all but two of the surveyed states-- work in North Carolina (see table 3).
| Adult blood lead cases, North Carolina, 1994 | |
| Blood lead level (µg/dl) | Total cases |
| Less than 25 | n.a. |
| 25-39 | 87 |
| 40-59 | 94 |
| 60-79 | 26 |
| 80+ | 17 |
| Total | 224 |
|
|
Since 1991, physicians and laboratories have been required to report adult (18 years old and above) blood lead levels of 25 µg/dl or greater to their local health department. All blood lead level reports must include a referring physician's name, address, and phone number. The local health department then forwards the reports to the Oregon ABLES registry located in the Oregon Health Division. However, most reports go directly from the laboratories to the Oregon Health Division. Three of the five major blood lead laboratories voluntarily report all blood lead levels. Out-of-state laboratories are also required to report. Although there is no enforcement mechanism, most of the large, national laboratories comply. ABLES funding supports 16% of a research analyst's time to maintain the database of blood lead levels and 12% of an industrial hygienist's time for follow-up activities.
Blood Lead Levels
In 1993, a total of 778 adult blood lead reports (representing 231 cases) of 25 µg/dl or greater were received. The source of exposure was known for 84% (194) of these cases. Where exposure history was know, occupational exposure accounted for 99% (192) of the cases. Of the occupationally related cases, 5.7% (11) were from the construction sector. One case greater than 40 µg/dl was construction-related; 612 of the reports were for workers in one battery manufacturing plant.
In 1994, the registry received 679 reports representing 271 cases. The source of exposure was known for 97% of these cases. Occupational exposure accounted for 97.3% (256) of those cases where exposure history was known. Of the occupationally related cases, 7.8% (20) were from the construction sector and 30% of the construction-related cases had blood lead levels of 40 µg/dl or above. The number of cases at 40 µg/dl or greater more than tripled from 1993 to 1994, while the total number of cases increased by 17%.
Follow-up Protocol
If registry staff determine that the lead exposure accounting for a report is occupationally related, the follow-up protocol is as follows:
- Blood lead level 25 - 39 µg/dl - The registry industrial hygienist sends a letter to the physician requesting that the physician provide lead-related information to the individual involved. Registry staff have not investigated whether physicians communicate such information to the patient. Case follow-up activities involving the referring physician are complicated by the practice of health care organizations using physicians who travel from one rural community to another.
- 40 - 49 µg/dl - The registry industrial hygienist contacts the referring physician.
- 1. The physician is given general information about the Oregon Lead in Industry and Lead in Construction standards and the industrial hygienist summarizes lead-related medical guidelines including testing-frequency requirements. Information on case management is gathered and the physician is asked for permission for the industrial hygienist to contact the patient directly.
- 2. If physician grants permission, the registry industrial hygienist contacts and interviews the patient regarding symptoms, activities on and off the job, and personal habits. Information about lead and lead exposure prevention is provided by phone and mail.
- 3. If the patient agrees, the registry industrial hygienist will contact the employer and provide the employer with exposure prevention information. Site investigations are not conducted by the staff industrial hygienist due to lack of resources.
- 50 µg/dl or greater - In addition to the above, the registry reports case information to Oregon OSHA (OR-OSHA) via a written quarterly report.
Referrals to OSHA
Currently, there is no formal agreement between the registry and Oregon OSHA. As per verbal agreement, employers having one or more workers with blood lead levels of 50 µg/dl or above are reported to Oregon OSHA on a quarterly basis. The registry reports approximately 10 to 12 reports per year to Oregon OSHA by this method. Oregon OSHA is not required to take action on these cases and, in most cases, it does not. If a physician or an employee requests a referral to Oregon OSHA, or a specific situation is of concern to registry staff, the registry will refer the case to Oregon OSHA immediately. These special referrals represent fewer than 5 cases per year. The registry tracks cases referred to Oregon OSHA and may be informed of Oregon OSHA's response to referrals. Oregon OSHA may also inform the registry about workplaces where workers are exposed to lead.
Construction Initiatives
Registry efforts are currently focused on storage battery manufacturing, primary metal manufacturing, and automotive repair shops (radiator repair). Although staff are aware of the lead hazard in the construction sector, there is no special surveillance of structural steel repair and repainting work. According to the Federal Highway Administration, Oregon has 1,789 deficient bridges (see table 3). In 1994, Oregon received $35.8 million in federal bridge funds and had 61,600 construction workers.
| Adult blood lead cases, Oregon, 1993 | |||||
| Blood lead level (µg/dl) | Construction | All other occupations | Unknown | Non-occupational | Total cases |
| Less than 25 | n.a. | n.a. | n.a. | n.a. | n.a. |
| 25-39 | 10 | 175 | 30 | 1 | 216 |
| 40+ | 1 | 6 | 7 | 1 | 15 |
| Total | 11 | 181 | 37 | 2 | 231 |
| Adult blood lead cases, Oregon, 1993 | |||||
| Blood lead level (µg/dl) | Construction | All other occupations | Unknown | Non-occupational | Total cases |
| Less than 25 | n.a. | n.a. | n.a. | n.a. | n.a. |
| 25-39 | 14 | 195 | 8 | 5 | 216 |
| 40+ | 6 | 41 | 0 | 2 | 49 |
| Total | 20 | 236 | 8 | 7 | 271 |
|
|||||
Occupational Health Program Adult Blood Lead Registry
Pennsylvania has required laboratories to report adult blood lead levels to the Department of Health since 1975, although the registry has been staffed only since 1992. Out-of-state laboratories are required to report lead levels of Pennsylvania residents, but effective enforcement mechanisms have not been discovered to assure compliance with this requirement. The Department of Health's Occupational Health Program administers the registry and carries out its intervention activities. Pennsylvania's adult blood lead reporting threshold is 25 µg/dl or greater for anyone over age 16 and 15 µg/dl or greater for pregnant women.
Blood Lead Levels
In 1993, the registry received a total of 6,139 reports (the number of cases was not available). A total of 5,971 of these reports were equal to or greater than 25 µg/dl. In 1994, 6,976 reports were received, of which 6,502 were equal to or greater than 25 µg/dl. While the number of reports increased at the lower levels (less than 40 µg/dl) and overall, reports decreased at the higher levels (greater than 40 µg/dl).
Because the Department of Health form submitted with the blood sample does not ask for the occupation of the individual, registry personnel do not know what share of these reports are due to occupational exposure or exposure to lead on construction sites. However, staff estimate that about half of the cases that the registry refers to OSHA (see below) are from the construction sector. The Department of Health form is being revised and the new form is expected to request information about the individual's occupation.
Follow-up Protocol
The program coordinator sends a letter with a brochure to all individuals (with addresses) who have a report of a blood lead level of 60 µg/dl and above. The brochure covers risk factors for occupational exposure to lead, the effects of exposure to lead, ways to avoid lead exposure, OSHA requirements, and sources of assistance. For extremely high-level reports (greater than 80 µg/dl), the program coordinator may make a follow-up phone call to the individual. Under certain conditions, the coordinator will report an employer to OSHA for further investigation.
Referrals to OSHA
Referral to OSHA is the primary direct intervention activity of the registry. Referrals to OSHA are made on a case-by-case basis. Factors influencing a referral include whether the employer is identifiable, how many elevated reports originate from that employer's worksite, and the extent of employees' elevated blood lead levels. Although there is no memorandum of understanding between OSHA and the Occupational Health Program, a cooperative relationship exists between the agencies. OSHA has pursued all referred employers and has sent a report to the registry after its visit to the referred employer's facility or site. Staff estimate that 50% of referred employers are in the construction sector.
Construction Initiatives
Although the registry does not have sufficient staff (the registry itself is a small part of the Occupational Health Program) to support a special emphasis program in construction, the program received NIOSH funding to organize two statewide lead-in-construction conferences for contractors and unions (see annex C). The Pennsylvania Department of Transportation (PENNDOT) and OSHA were cosponsors of the conferences, were represented on the planning committee, and were presenters at one of the conferences.
The registry program coordinator, an industrial hygienist, has been working to establish a relationship with the Pennsylvania Department of Transportation since 1994 and has been invited to participate in the department's bridge inspections, review lead-related contract specifications, and provide the Department of Transportation with written evaluation of her findings. Additionally, in 1995, the Occupational Health Program commissioned a focus-group survey of both industrial and construction workers entitled, "Knowledge, Attitudes and Experience about Occupational Lead Exposure among Pennsylvania Workers."
Pennsylvania leads the 13 surveyed states in bridges defined as deficient by the Federal Highway Administration (9,771) and in dollars for bridge repainting and repair ($257.1 million in 1994) (see table 3). The state has a seasonally adjusted average of 202,800 construction workers.
| Adult blood lead reports, Pennsylvania, 1993 and 1994 | ||
| Blood lead level (µg/dl) | 1993 Total reports | 1994 Total reports |
| Less than 25 | 168 | 474 |
| 25-39 | 4,098 | 4,837 |
| 40-59 | 1,704 | 1,602 |
| 60+ | 69 | 63 |
| Total | 6,139 | 6,976 |
|
||
South Carolina's Reportable Disease Law requiring the reporting of adult blood lead levels dates back to 1971. All blood lead test results must be reported, regardless of their level. The registry is located in the Department of Health and Environmental Control's Division of Health Hazard Evaluation. All laboratories, hospitals, and physicians are required to report blood lead levels.
Blood Lead Levels
In 1993, 1,248 cases were reported to the registry, 40% of which were equal to or greater than 25 µg/dl. In 1994, cases increased by over 100% to 2,588, although the share of cases greater than 25 µg/dl declined to 20% of the total. Because South Carolina's reporting requirements were instituted in 1971, the increase in cases from 1993 to 1994 is not likely to be due solely to increased compliance with reporting requirements. However, 1994 was the first full year of blood lead testing requirements under the OSHA Lead Exposure in Construction standard and it is possible that the dramatic increase in cases less than 25 µg/dl is due to the increased testing of this population. As with other states, cases in South Carolina at the highest levels -- greater than 60 µg/dl -- decreased 1993 to 1994. Registry staff have determined that 97% of cases reported to the registry are occupationally related, but the staff are not aware of any cases from the construction sector.
Follow-up Protocol
Registry staff attempt to contact all individuals having blood lead levels over 40 µg/dl. If phone numbers are available, registry staff conduct a telephone interview to determine the source of the exposure. If no phone number is available, a questionnaire is mailed to the individual. Educational materials on applicable laws, health effects, and control techniques are mailed to all cases over 40 µg/dl. Additionally, the registry reports the employers of cases over 40 µg/dl to OSHA.
Referrals to OSHA
Through an informal agreement with South Carolina OSHA, the registry refers the employers of workers with blood lead levels over 40 µg/dl to OSHA's Consultation and Training Division. Employers of cases over 50 µg/dl are reported to OSHA's Compliance Division.
Construction Initiatives
There are no programs focusing on the prevention of elevated blood lead levels in construction workers. In 1994, the Department of Health and Environmental Control held a conference on lead in construction that was well attended by construction workers. Although the problem has been acknowledged in departmental meetings, the prevention of lead poisoning in construction workers is not considered a priority for public health intervention efforts.
South Carolina has only 1,884 deficient bridges (compared to the 13-state average of 4,000), received $27.4 million in bridge repair funds in 1994, and has 84,300 construction workers, on average (see table 3).
| Adult blood lead cases, South Carolina, 1993 and 1994 | ||
| Blood lead level (µg/dl) | 1993 Total cases | 1994 Total cases |
| Less than 25 | 755 | 2,055 |
| 25-39 | 212 | 145 |
| 40-59 | 219 | 336 |
| 60+ | 62 | 52 |
| Total | 1,248 | 2,588 |
Lead poisoning, defined as a blood lead level of 10 µg/dl or greater, was added to Tennessee's list of notifiable diseases on November 28, 1995. Any laboratory, in or out of state, conducting a blood lead test on a Tennessee resident must report the results to the Tennessee Department of Health, Maternal and Child Health Section. Physicians are also required to report test results. Unlike the laboratory reporting form, the physician's report must include the reason for the test, the treatment provided, and the suspected source of exposure.
Blood Lead Levels
Data are not available on adult blood lead levels or on the occupations of adults whose blood lead levels have been reported.
Follow-up Protocol
Tennessee has 13 Department of Health administrative regions. The registry sends blood lead data to nurses in each of these regions. Follow-up activities primarily focus on children with blood lead levels 10 µg/dl or greater. Some intervention activities do target adults who are occupationally exposed to lead. If the regional nurse receives a report for an adult working in his or her administrative region, the nurse may contact the employer and offer to organize a health fair to distribute information and test workers' children.
Referrals to OSHA
The registry does not report cases to Tennessee OSHA.
Construction Initiatives
The registry does not have any initiatives in construction. Tennessee has 5,456 deficient bridges (surveyed states averaged 4,000 deficient bridges per state), received a relatively large amount of federal bridge money in 1994 ($60.7 million), and has an average of 101,200 construction workers (see table 3).West Virginia has 3,023 deficient bridges, received $54.4 million in bridge repair funds in 1994, and has only 34,100 construction workers, on average.
- When was the law passed?
- Who is required to report?
- Do you require
out-of-state laboratories to report adult blood lead levels of individuals
who reside in your State?
- a. If so, how is this enforced?
- Is it a requirement
to report all adult blood lead levels or is there a threshold below
which labs/physicians are not required to report blood lead levels?
- a. If so, what is the threshold?
- Does your department
report elevated adult blood lead levels to OSHA? Is it done routinely
or is it done on a case by case basis?
- a. If reporting is done through a formal agreement with OSHA, what year did this go into effect?
- What kind of
action is taken by DOH upon receipt of reports of elevated adult blood
leads (e.g. none, phone interviews, industrial hygiene evaluations,
inspections)?
- a. What triggers action?
II. We are particularly interested in blood lead levels reported for workers employed in the construction industry as compared to the total number of adult blood lead levels reported. In addition, we are interested in any special initiatives which have been developed to target this industry.
1. Please fill out the following table for 1993 and 1994 as completely as possible. For each of these years, please identify the highest blood lead level (µg/dl) for each reported case (not report.) By case we mean each individual, since an individual may have more than one blood lead level report per year, depending upon the number of times they have been tested.
If no occupational breakdown is available, please provide the total number of adult blood lead cases reported for each of these two years.
1993
| Blood lead level (µg/dl) | Construction | All other occupations | Unknown | Non-occupational | Total |
| Less than 25 µg/dl | |||||
| 25-39 | |||||
| 40-59 | |||||
| 60-79 | |||||
| 80+ | |||||
| Total |
1994
| Blood lead level (µg/dl) | Construction | All other occupations | Unknown | Non-occupational | Total |
| Less than 25 µg/dl | |||||
| 25-39 | |||||
| 40-59 | |||||
| 60-79 | |||||
| 80+ | |||||
| Total |
2a. If you do not have the information to complete the above tables, do you know or can you estimate the percentage of blood lead level cases that are occupationally related?
- Yes No
- % occupationally related:
- number of cases occupationally related:
- b. Do you know or can you estimate the percentage of the occupationally related cases that are in construction?
- % construction related:
- number of cases construction related:
If yes,
c. What is the basis for your information or estimates?
3. Are elevated blood lead levels from a construction setting handled differently from other occupationally related elevated blood lead levels?
- Yes No
- If yes;
- a. What triggers reporting?
- b. Who is required to report to what agency/entity?
- c. What kind of action is taken, e.g. none, phone interviews, industrial hygiene evaluations, inspections?
- d. What triggers action?
4. Is there any surveillance program or activity for lead specific to construction?
- If yes, please answer the following questions.
- a. When was this program/activity started?
- b. Does the program/activity have a special focus on steel structures, residential settings, commercial buildings or other settings?
- c. What agencies and/or institutions are involved (such as Department of Transportation, Department of Health, Occupational Safety and Health Administration, Department of Environmental Protection)?
- - Describe the responsibilities of the agencies/institutions involved.
- d. How is it funded and what is the annual funding amount?
- e. Does your department have staff dedicated to this construction emphasis program?
- Yes No
- f. Does the Department of Transportation or any other agency have separate contract specifications which deal with worker lead health programs in construction?
- Yes No
- if so, what type of work is covered?
- I. Do the contract specifications require the contractor to report blood lead levels to the registry or other entity (e.g. DOT)?
- If yes, who is required to report and where do they report?
- II. Please describe the worker health provisions of the contract specifications such as medical surveillance, industrial hygiene evaluation and intervention, lead health programs, enforcement, etc.
- III. Could you send us a copy of the contract specifications?
- g. Does the DOH/registry have a Memorandum of Understanding or other type of arrangement with the DOT or other agency regarding lead in construction activities?
- If yes, please
describe:
- type of arrangement/agreement
- how the DOH/registry and DOT/program interface
- in-kind staff for data collection and/or intervention
- agreement on protocols for medical surveillance, inspections, interventions
- special reporting requirements to DOH (who reports - DOT, contractor)
- use of DOH industrial hygiene staff
- h. Are there any additional elements of this program that we have not covered? Please describe.
- i. Is there any other mechanism by which DOH and/or the registry is informed about blood lead levels in construction? If so, please describe.
- Please specify job title and time allocated (i.e. clerk - part-time, industrial hygienist- full time, etc.)
Yes No
Yes No
5. If the DOH/Registry does not have a construction emphasis program for blood lead level surveillance and intervention:
- Is one under consideration?
- What kinds of problems are you facing in starting such a program?
6. Did your State have a lead in construction standard which preceded the federal OSHA Interim Standard of April, 1993?
- If yes, could you please send us a copy?
7. Do you have medical
questionnaires, lead exposure occupational history questionnaires, outreach
materials, etc. used as part of your medical surveillance program? Could
you send copies to us?
8. Would you be
interested in reviewing the report summarizing the information we collect
from this survey?
Note: The following Samples have available as images which can be viewed by clicking on the following 5 links.
Page 1 | Page 2 | Page 3 | Page 4 | Page 5
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Alabama
J.P Lofgren, M.D., State Epidemiologist
Division of Epidemiology
Alabama Dept. of Public Health
434 Monroe Street
Montgomery, AL 36130-3017
Phone: 334-613-5347
Fax: 334-288-5021
Alaska
Grace Egeland, Epidemiologist
Alaska Dept. of Health
Section of Epidemiology
3601 C. St., Suite 540
Anchorage, AK 99524-0249
Phone: 907-269-8000
Fax: 907-561-6588
Florida
Raul Quimbo, MBS
Florida HRS/HSEE
1317 Winewood Blvd
Tallahassee, FL 32399-0700
Phone: 904-488-3370
Fax: 904-922-8473
Idaho
Donna Julian, Program Coordinator
Idaho Blood Lead Registry
Idaho Dept. of Health and Welfare
450 W. State St.
Towers Building, 4th Fl.
Boise, ID 83720-0036
Phone: 208-334-6584
Fax: 208-334-6581
Indiana
Bill Letson or Dr. Greg Steel
Indiana Department of Health
Epidemiology Resource Center
2 North Meridian St., 3rd Fl.
Indianapolis, IN 46204
Phone: 317-233-7207
Fax: 317-233-7378
Kentucky
Pat Beeler
Cabinet for Health Services
Department for Public Health, Division of Epidemiology
Surveillance and Investigations Branch
275 East Main Street
Frankfort, KY 40621-0001
Phone: 502-564-3418
Fax: 502-564-4553
Mississippi
Pam Nutt
Div. Of Child and Adolescent Health
Mississippi Dept. of Health
Box 1700
Jackson, MS 39215-1700
Phone: 601-960-7476
Fax: 601-354-6087
North Carolina
Bill Jones
North Carolina Dept. of Environment, Health and Natural Resources
Occupational and Environmental Epidemiology Section
Dept. of Occupational Health Surveillance
Box 27687
Raleigh, NC 27611-7687
Phone: 919-733-1145
Fax: 919-733-9555
Oregon
Narda Tolentino, Program Manager
Environmental, Occupational, and Injury Epidemiology
Oregon Health Division
800 NE Oregon Street
Suite 730
Portland, OR 97232
Phone: 503-731-4025
Fax: 503-731-4082
Marilyn Scott, Industrial
Hygienist
Lead Program: Environmental, Occupational, and Injury Epidemiology
Oregon Health Division
800 NE Oregon Street, Suite 730
Portland, Oregon 97232
Phone: 503-731-4025
Fax: 503-731-4082
Pennsylvania
Judy Gostein, MS
Industrial Hygienist
Div. Environmental Health Assessment
Pennsylvania Dept. of Health
Box 90, Room 1020
Harrisburg, PA 17108
Phone: 717-787-1708
Fax: 717-783-3794
South Carolina
Annette Gardner, Project Administrator
Division of Health Hazard Evaluation
Dept. of Health & Environmental Control
2600 Bull St.
Columbia, SC 29201
Phone: 803-737-4173
Fax: 803-737-4171
Tennessee
Marilyn Holmes, Coordinator
Childhood Lead Poisoning Prevention Program
State of Tennessee Dept. of Health,
Maternal and Child Health Section
426 Fifth Avenue North
Cordell Hall Building, 5th Floor
Nashville, TN 37247
Phone: 615-532-7778
Fax: 615-741-1063
West Virginia
Linnea Ohgren
Div. Of Surveillance and Disease Control,
West Virginia Bureau of Public Health
Dept. Of Health and Human Resources
1422 Washington St. E.
Charleston, WV 25301
Phone: 304-558-5358
Fax: 304-558-6335
Dr. Nawal Lutfiyya
Office of Maternal and Child Health
Division of Research, Evaluation and Planning
1411 Virginia St. E.
Charleston, WV 25301
Phone: 304-558-7996