
Summary Statement
An article about the dangers of silica, attempts being made to change regulations to improve safety, and ongoing research on training and new technologies to help in prevention
November 6, 2000
Kids play in it, masons mortar with it, painters blast with it and operating engineers push it around with equipment. Sand and other aggregates containing silica can be benign and productive building materials when used properly, but they can be slow and silent killers when workers on construction sites and in quarries chronically breathe the airborne dust from the products. The resulting silicosis is an ancient disease that causes scarring in the lungs, reduced lung capacity, heart problems and even death.
Silica is the basic component of sand, quartz and granite and is found just about everywhere in varying proportions. It accounts for 12% of the earth's crust by weight and is found in the aggregates, sand, mortar, concrete and stone that construction workers routinely come in contact with. It also is in the air and the soil. The dangerous kind is crystalline silica, or silicon dioxide (SiO2). Because of the varying proportion of crystalline silica in rock and the dynamic exposure that workers have to the material in construction, hard data on exposure is hard to find or calculate. But health experts estimate that thousands of construction workers are exposed each year and that at least 250 workers in all industries die annually from silicosis.
The disease is similar
to asbestosis in that it sometimes takes years to manifest itself, is
difficult to diagnose and can be prevented with the proper personal protective
equipment or engineering controls. "Inhalation of fine particles
of crystalline silica produces a scarring in the lung [that] acts as a
barrier and causes difficulty in moving air in and out and prevents getting
oxygen into the blood stream," says Dr. Stephen Levin, medical director
of Mt. Sinai Irving J. Selikoff Center for Occupational and Environmental
Medicine, New York City. "The more dust inhaled, the more scarring
there is."
Heart disease is a companion problem. "Silicosis can destroy blood
vessels that run through the lung and cause back pressure on the right
side of the heart," which is the side that pumps blood to the lungs,
says Levin. Silicosis "will stiffen lungs, narrow airways and cause
shortness of breath and coughing. In severe cases, victims end up with
pulmonary impairment to the point that they have to go on oxygen."
How much silicosis people will develop depends on genetics and degree
of exposure to respirable quartz, which is silica dust ranging from .2
or .3 microns in diameter to 5 microns, says Levin. Particles larger than
this are trapped in upper airways and smaller particles are largely blown
out because they act like a gas, he says. Nonetheless, Levin believes
that even the smallest particles have a biologic impact.
Levin says the genetics angle is not well understood. "Two people
can work side by side [in silica conditions] and in one, there will be
scarring, and in the other, the scarring will be nominal," he says.
"But you can't do genetic testing on people before you send them
out [to a jobsite] and "if there is enough dust, everybody gets some
[scarring]."
Specter. And there
is a more ominous specter. In 1996, the International Agency for Research
on Cancer in a controversial decision concluded that "there was sufficient
evidence" to categorize certain kinds of silica as a carcinogen.
"That was the trigger for the Occupational Safety and Health Administration
to look at it again," says Charles E. Hawkins III, executive vice
president of the newly merged National Aggregates Association-National
Stone Association, Arlington, Va. "The bottom line is that we had
a European group decide that it was a carcinogen with no studies."
Others believe concern is justified. "It looks as if crystalline silicosis carries with it an increased risk of lung cancer," says Levin. "We are concerned [and] there is enough evidence now to suggest it. The best thing is to protect workers."
In 1996, former Secretary
of Labor Robert Reich kicked off an OSHA special emphasis program for
silica to educate the industry about silica exposure and start the wheels
moving for a new construction standard. "It is a direct result of
that initiative that we are undertaking rulemaking," says Berrien
Zettler, deputy director of OSHA's Construction Industry Directorate in
Washington, D.C.
In the short term, OSHA is working with the National Institute for Occupational Safety and Health to develop a metric conversion factor that will allow OSHA to resume enforcing the existing OSHA standard for construction. "It is a very old standard" from the 1960s that preexists OSHA, and it contains an "obsolete sampling standard so there is no way we can legally measure or enforce it," says Zettler. The standard measures silica in terms of millions of particles per cubic feet of air and monitoring devices using that measurement no longer are manufactured. The new metric conversion factor "will allow us to issue citations if the exposure is high enough," even if we miss some marginal exposures, he adds. The Labor Dept.'s Solicitor's Office is reviewing the matter and approval is expected by mid-November. That is a bit uncertain because of the "highest priority" that the agency now is giving its controversial proposed construction standard for ergonomics.
In the longer term, OSHA is moving toward the adoption of a new construction standard, which Zettler hopes to have in proposal form by the end of next year. The agency has been having a series of meetings for "stakeholders" to voice their positions. The next one is scheduled for Nov. 8-9 in Atlanta.
According to Zettler, there are still a number of open scientific questions that will affect the rulemaking process and the permissible exposure level, including the carcinogenic nature of silica. When dealing with carcinogens, "we are required to regulate that to the lowest possible level" by agency policy, he says.
Therein lies the problem for a group of 17 companies and organizations that banded together as the Silica Coalition when OSHA announced its silica initiatives in the mid 90s. "We want to make sure that the new regulations are based on sound science," as well as economic impact studies, says coalition chairman Robert E. Glenn, a certified industrial hygienist who also is president of the National Industrial Sand Association, Calverton, Md. The coalition is supporting a number of studies now under way relating to the link between silica exposure and silicosis, he says. "We will have new data by the time OSHA comes up with a new rule." Glenn adds: "We are not opposed to a standard as long as the science is clear and the exposure limit is a correct one that protects workers." Preliminary talks also are under way with OSHA about the possibility of having a negotiated rulemaking, he says.
OSHA wants to cut the permissible exposure limit in half, and "we have put out advisories to our members," says Bradley Sant, director of safety and regulatory affairs for the American Road and Transportation Builders Association, a Silica Coalition member. "As an association, we are concerned about the impact" of that kind of change, he says.
Standing in the corner of craftworkers are the building trade unions and CPWR – Center for Construction Research and Training, the safety and health arm of the AFL-CIO's Building and Construction Trades Dept. "In terms of life-years lost, silicosis is a bigger problem than asbestosis," says Pam Susi, an industrial hygienist who is director of the CPWR's Exposure Assessment Program. She notes that silicosis takes less time to develop and workers are dying at a much younger age, some in their 40's with less than five years of exposure.
The flurry of recent
activity makes silicosis look like a new discovery, but it is not. "Silicosis
has been known as long as mining has gone on," says Mt. Sinai's Levin.
In one of the worst U.S. industrial disasters, more than 400 and maybe
as many as 2,000 construction workers died of silicosis after digging
a three-mile-long hydroelectric tunnel through almost pure silica in Gauley
Mountain, W. Va. in 1930-32. The contractor chose dry drilling over wet
because it thought it would save time. Workers developed acute cases of
silicosis and began dying within months of the first symptoms.
Despite such lessons, progress has been painfully slow. "We hear about guys in their 40s dying now from an ancient disease. It is appalling," says Susi of CPWR, which is conducting exposure studies. Construction trades that are potentially directly exposed to silica include rock drillers, sandblasters, laborers, masons, operating engineers and others that might disturb the material. But once the dust is created on a jobsite, it affects everyone, including people just passing by.

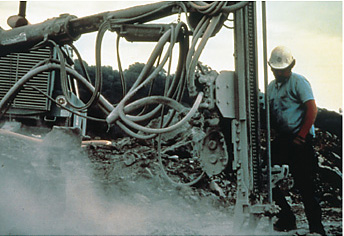
As might be expected,
sandblasters using silica sand are among those most at risk if they are
not using the proper personal protective equipment and engineering controls.
Tests now are under way at NIOSH to assess the blast alternatives to sand.
NIOSH tested 40 blast products to determine their effectiveness and toxicity. Sand is still the most widely used because "it's cheap, it's available and it works reasonably well," says Mark Greskevitch, a NIOSH industrial hygienist who ran the study in Morgantown, W. Va. The only problem is that it causes silicosis because "people are not using state-of-the-art personal protective equipment or engineering controls."
NIOSH looked at 10 materials and measured them for productivity and 30 elements of respirable dust when blasted against uncoated steel plate at about 100 psi of air pressure in the lab and in the field. In terms of respirable quartz, "sand was humongous" says Greskevitch. Other blast materials tested included crushed glass, specular hematite, coal slag, copper slag, nickel slag, steel grit, olivine, garnet and staurolite. However, the tests indicated that there were some other hazards present in the alternative materials. For example, coal slag dust contained arsenic--"enough to worry about," says Greskevitch. Copper slag had it as well. Steel grit was low in toxicity as well as dust, as was specular hematite.
"The technology is there for sandblasters to use air-supplied hoods," says Mike Damiano, director of product development for sspc--Society for Protective Coatings (formerly Steel Structures Painting Council), Pittsburgh. "Years ago, they probably put a handkerchief over their head." He notes that some industrial owners will not allow silica sand in their plants.

"Many contractors
don't care, or care only as much as the facility owners make them care,"
says James D. Hansink, chairman of SSPC's abrasives committee and president
of consulting firm Garnet Services Inc., Seattle. The problem is being
exacerbated because major industrial owners are contracting out to private
firms work that they used to manage in-house and they are rewarding purchasing
agents who get low prices, he says. Contractors err by using sand "because
they think that this is the only way they can be competitive," he
adds. "They measure costs in dollars per ton rather than dollars
per square foot cleaned," he adds.
Bricklayers are at risk because of tools and work practices. "I've lost enough men. I know about it," says Frank Stupar, recently retired executive vice president of the bricklayers' union and former chairman of the BCTD's silica subcommittee. "Even if your people are not generating the dust, it is doing the job with you or without you."
Stupar's top target is gas-powered chop saws used to dry-cut brick and block. He and the union developed model contract language so that locals could "negotiate that junk right out of our agreements." So far, the chop saws are banned in Massachusetts, Detroit and some locals in Pennsylvania, among others. "We have had great success with contractors' in suppressing the dust hazard through the use of wet cutting of masonry," says Stupar. "Water, for Christ's sake, it is cheap enough. They recognize the potential liability." Stupar says the building trade unions are drafting a model silica standard for construction that they will submit to OSHA for consideration.
The bricklayers' union and NIOSH also are studying ways to make the grinding out of mortar during tuck pointing of masonry more dust free. "We can't really have a standard until we have a solution," says Clarence Nichols, deputy director for regional training at the International Masonry Institute's national training center at Ft. Ritchie, Cascade, Md.
Union bricklayers build a 13-ft-long, 8-ft-high standard brick wall at Ft. Ritchie for NIOSH to test a group of commercially available shrouds and vacuums hooked to standard 4.5-in grinders. The wall was enclosed in a chamber and the grinders were run down the wall mechanically on a carriage and track system. A diamond blade on the grinders removed .5 in. of mortar while computers measured the particulars produced.
"It looks like there are some real good dust controls available," says William Heitbrink, a NIOSH research chemical engineer and industrial hygienist based in Cincinnati, who ran the test. Heitbrink says the full results won't be ready for a month, since the testing has just ended. However, he says the critical performance characteristic is the amount of suction that the HEPA vacuums can generate, noting that they need about 100 cfm for the 4.5 in. grinder. And work practices also are critical because the shape of the receiver hood/shroud and blade allow dust to be collected effectively only while the operator moves the grinder in one direction while keeping the blade imbedded in the mortar.

Heitbrink also tested the grinders with a 3/8-in router bit designed for removing mortar. He says the vacuum flow could be reduced by 50% and still be effective because "there is less induced air flow" from the bit than from the larger blade. "We are making progress on this," he concludes.
"You could definitely see a significant reduction in dust," says Robert F. Herrick, an industrial hygienist and senior lecturer at Harvard University, who worked with Boston bricklayers in testing another version of the dust-collection system that was built from scratch. "The technology has to be refined so that it works in the real world [but] there is a definite need for these kinds of controls," says Herrick. "They are inevitable."

Mt. Sinai currently is working on a CPWR surveillance project to measure the silica exposures of bricklayers and laborers using pneumatic jackhammers, drills and chippers on roadways, bridges and transportation centers in the New York City area. "The exposures we are seeing are quite high--90% above OSHA exposures and NIOSH's recommended standard," says Mark Goldberg, an industrial hygienist and assistant professor at the medical center. Taken at random, and worker engaged in these activities is being exposed unless protected, and "I still go out to jobsites and see workers not wearing dust masks," he says. "There is a lot of infrastructure work going on now, but no widespread surveillance."
The painters' union is working with the New Jersey Dept. of Health to monitor exposure of members to silica. At the moment there is a lot of bridge work going on and the union wants "facts and figures on real jobs," says Jerry Taggart, safety and health instructor for statewide painters' union district Council 711. On one recent monitored sandblasting job, the silica exposure was 225 times over the permissible exposure limit, but the worker was fully protected.
The N.J. Health Dept. also has drafted a medical document that construction workers can give to their doctors alerting them to the possibility of exposure to silica on the job and the possible consequences of it. The document offers suggestions on various tests to perform to diagnose silicosis and notes that New Jersey and many other states require that cases be reported to the health department so that it can determine whether employers are controlling silica exposure.
The medical alert is essential because underreporting and misdiagnosis of silicosis is widespread, says Scott Schneider, director of occupational safety and health for the Laborers' Health and Safety Fund, which is distributing copies. In one study, an X-ray reader experienced in silicosis looked at the X-rays of a number of people who died of lung disease and found that many were never diagnosed with silicosis, he says.
Getting construction workers themselves to recognize the dangers of silicosis exposure is sometimes difficult because they think it is just sand. "You don't know what is in dust just by looking at it," says Frank Hearl, deputy director of NIOSH's Division of Respiratory Disease Studies in Morgantown. "Don't put yourself at risk," he says, noting that the disease is incurable and progressive. "You can't turn back the hands of time after you've got it."