
Injuries Are Not Accidents: Construction Will Be Safe When It's Designed to Be Safe (Case Study 4 from Lessons Learned - Solutions for Workplace Safety and Health
Summary Statement
Case study on hazardous conditions and actions that could be taken to prevent these conditions, including implementing an occupational safety and health management system in the worksite.
 This welder looks about as well protected as could be. But real safety requires more than personal protection equipment. Safety in construction means planning and managing every aspect of a site with safety in mind. |
| On August 13, 2005, a 56-year-old male construction worker was fatally injured when he was run over by a bulldozer. He had been working at a commercial construction site in North Carolina. As he stepped in front of a gravel pile to direct a truck driver, he was struck by a bulldozer running in reverse. His boss, the owner of the contracting company, was operating the bulldozer, spreading gravel. The dozer’s back-up alarm was on. A co-worker in a skid-steer loader near the gravel pile saw the bulldozer backing toward the victim, and he yelled a warning. But neither the driver of the bulldozer nor the worker in its path heard him shout. The track of the bulldozer struck the victim on the back of his legs and rolled over his legs and torso. Emergency medical workers arrived promptly after the 911 call and found that the victim had no signs of life. He was pronounced dead at the site. |
| — Fatality Assessment and Control Evaluation (FACE) Program, National Institute for Occupational Safety & Health (NIOSH)1 |
Unnecessary deaths like this one happen all the time—there are approximately three fatal construction injuries each day in the United States.a And for every death, there are more than 100 nonfatal injuries serious enough to result in time lost from work.b
Fatal injuries in construction continue to take a heavy toll despite a long history of government efforts to enforce safety measures. Yet safety management systems involving workers and managers in continuous assessment and prevention can provide the commitment to safety that is critical to reducing deaths and injuries on the job.
When people hear about these tragic and avoidable deaths, they often have one of two reactions. They either say, “It should be so simple—how hard can it be to keep workers from falling, or being crushed, or being electrocuted?” Or they say, “Accidents will always happen. It’s nobody’s fault.” The latter view is clearly wrong, and the evidence can be found in very safe construction projects all over the world, even if they are not as common as they should be. The first view is also wrong, but in a subtler way. The final error that leads to the injury or death—the bulldozer running over the worker— may be simple to avoid when viewed in isolation. However, keeping workers safe requires careful, participatory design of the organization of work practices and the worksite. Investigations of fatal injuries invariably find a complex web of causal factors that led up to the final moments of the terrible, avoidable event.
This case study highlights the complex, very hazardous, and often fast-paced work of construction, an industry that is also known to employ a vulnerable population of immigrant workers. To manage its countless occupational hazards and protect workers adequately, the construction sector requires a more comprehensive approach than mere compliance with government standards or sporadic application of control measures after serious incidents occur. One of the best solutions is to implement an occupational safety and health management system (OSH-MS) in the worksite.
The highly hazardous construction sector
A complex and dynamic work environment
The construction industry is one of those complex economic sectors that pose particular challenges in protecting workers’ safety and health.2 Construction work embraces not only building projects but also maintaining, repairing, renovating, and demolishing houses, apartment buildings, and office buildings. Larger-scale construction projects include not only major buildings (for example, health care facilities), but also infrastructure components (e.g. roads, tunnels, bridges, airports, docks).2,3 In these various activities, the worker experiences highly hazardous conditions— not only the hazards of his/her own job, but also hazards from co-workers.2,3 Construction workers also operate in an unusually dynamic workplace: construction requires the physical transformation of the site: each new stage of the project brings along different materials, technologies, work processes, and hazardous exposures.4
Dangerous job conditions may include work at heights or in excavations; the clutter of building materials; motor vehicles and equipment; prolonged standing, bending and stooping; noise, dust, and welding fumes; power tools; confined spaces and cramped spaces; temperature extremes; electricity; and sometimes work underwater. Other features of construction work that may contribute to hazardous conditions include working at a fast pace, having many employers on the site, working jobs of relatively short or episodic duration, and working alongside trades that generate other hazards.3 Furthermore, construction workers are highly mobile and employers may change. All these factors make the documentation of construction jobs and hazardous exposures complex.2 When employed, most workers in the construction industry work at least full time and many of them more than 40 hours a week.5
About This Case Study The first section of the case study profiles the chief characteristics of this hazardous employment sector: number of injuries, especially hazardous trades, costs of construction injuries, and the magnitude of the immigrant workforce and the nature of its work. The second part highlights actions by government and the construction industry that could make this sector safe. |
Construction industry tops the injury numbers
Workers in the construction sector are about 8 percent of the US workforce (more than 11 million workers), but the industry consistently accounts for a larger number of total fatalities than any other sector—accounting for about 22 percent of fatalities across all industries.6 In 2008, the Bureau of Labor Statistics (BLS) reported 975 deaths from acute traumatic injuries.7,8 The 2008 fatality rate, at 9.6 deaths per 100,000 full-time construction workers, was the fourth-highest after agriculture, mining, and transportation.8 Although preliminary BLS data indicate that construction fatalities declined to 816 in 2009,9 the construction industry continues to top the list of highfatality industries.
The leading causes of construction fatalities and injuries, accounting for 90 percent of cases, are:10,11
- falls from elevations (e.g., from floors, platforms, ladders, roofs);
- being struck by something that is moving (e.g., objects, pieces of equipment, vehicles);
- being caught in/between events or objects (e.g., cave-ins, unguarded machinery, equipment); and
- electrical shock (e.g., by overhead power lines, power tools and cords, outlets, temporary wiring).
Falls are the most frequent cause of fatalities in construction, each year accounting for one-third of all construction-related deaths.12 The proportion is higher in residential construction, where falls account for nearly half of work-related deaths.13 Figure 1 shows trends of construction fatalities for falls, highway accidents, contact with electric current, and being struck by objects during 1992–2005.14
In 2008, BLS reported that the construction industry experienced a total of 120,240 serious nonfatal injuries causing days away from work (11 percent of such injuries across all industries); this is the fourth highest percentage among all US industry sectors, behind trade, transportation and utilities (30 percent); education and health services (17 percent); and manufacturing (13 percent). 15 Construction sector injuries causing days away from work had the highest lost-time rate (174 injuries per 10,000 full-time workers) of any US industry sector.15
Studies of non-fatal construction-related contact injuries (that is, injuries in which a worker is struck by an object or a piece of equipment) treated in emergency departments during the period 1998–2005 found that contact injuries accounted for over half of all construction injuries treated in emergency departments.16,17 The most common injuries were due to contact with discharged nails from pneumatic nail guns, hand-held power saws, and fixed saws.16 Some injuries may involve multiple workers (e.g., trench cave-ins, collapses of walls, roofs, or scaffolding of buildings under construction).16 Seven specific tools or pieces of equipment—ladders, nail guns, power saws, hammers, knives, power drills, and welding tools— were responsible for almost two-thirds of the injury burden in emergency departments.17
Construction workers suffer not only occupational injuries, but also numerous occupational illnesses. Many of these illnesses are difficult to capture in statistics because of long latencies, as described below.
Among the many trades and occupations involved in the construction industry roofers, along with structural iron and steel workers, were the trade groups suffering from both the highest rates and largest numbers of fatal injuries in 2008.8 Construction laborers were the largest group suffering from non-fatal injuries in 2008.15
Injuries are not the only risk: occupational illnesses of construction workers
Figure 1: Leading causes of work-related deaths in construction, 1992–2005.
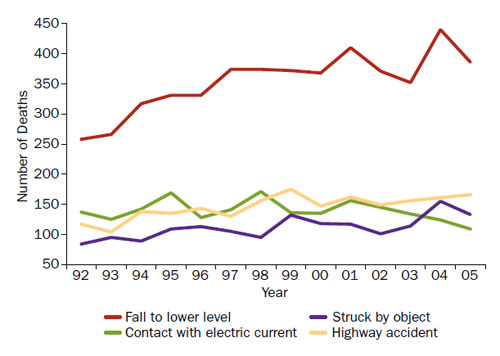
Source: CPWR - The Center for Construction Research and Training. The Construction Chart Book. 2008. Chart 36c, p36.
Several specific work-related diseases have been associated with working in the construction trades, including these:
- lung cancer among asbestos insulation workers, roofers, welders, and woodworkers;3,18-21
- silicosis among sand blasters, tunnel builders, rock drill operators, masonry and concrete workers, and workers in other trades;3,13,18,22-31
- asbestosis and mesothelioma among asbestos insulation workers, steam pipe fitters, building demolition workers, and sheet metal workers;3,13,20,32-35
- chronic obstructive pulmonary disease (COPD) among cement masons, brick masons, plasterers, sheet metal workers, and welders;13,21,36,37
- skin diseases among laborers who work with cement or concrete, masons, tile setters, terrazzo workers, painters, and others;3,38-45 and
- neurologic disorders among painters, welders and other workers exposed to organic solvents and metals (e.g., lead, chromium, manganese).3,13,46-52
Figure 2: Rate of back injuries and illnesses per 10,000 full-time (FT) workers with days away from work, by selected construction occupation in 2005.
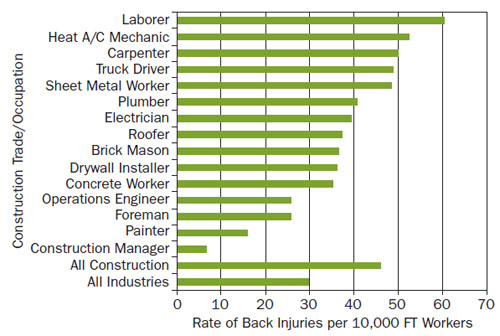
Source: CPWR - The Center for Construction Research and Training.
The Construction Chart Book. 2008. Chart 16b, p16.
Welch and colleagues have examined in some depth the risk of asbestos-related lung disease among sheet metal workers, studying more than 18,000 workers with more than 20 years’ work experience who had been screened between 1986 and 2004.35 At the first screening, almost 10 percent had asbestosis and 21 percent had scarring of the pleura (the lining of the lungs). A second exam, given an average of 10 years later to those with no evidence of asbestos-related lung disease on first exam, found that more than 5 percent had developed asbestosis and more than 12 percent had developed pleural scarring.35 Lead poisoning has been documented not only among painters but also among building finishing workers, street and bridge rehabilitation workers, and utilities workers.3,13,46-48 Asthma, neurological disorders (e.g., manganeseinduced Parkinsonism), and cancer have been documented among welders, who are exposed to a variety of metal fumes, including manganese and iron.49-52
Musculoskeletal disorders
Schneider carried out a comprehensive review of musculoskeletal injury evidence in construction— the study showed that construction workers are at significant musculoskeletal injury risk.53 The evidence review included the following data sources: (1) historical evidence; (2) injury data (e.g., BLS data); (3) workers’ compensation data; (4) medical exam data; (5) worker symptom survey data (e.g., National Health Interview Survey data); and (6) job exposure analysis data.53
In the ergonomics case study of this publication, we present the BLS 2008 data on the top five occupational groups for musculoskeletal disorders (see Table 1 of the case entitled When My Job Breaks My Back: Shouldering the Burden of Work-Related Musculoskeletal Disorders).15 The construction and extraction occupations were among the top five groups. Overexertion is the leading cause of musculoskeletal disorders (MSDs) in construction.14 For construction and extraction occupations, the 2008 BLS data indicated that arm and shoulder MSDs resulted in the highest number of days away from work in construction.15 However, the incidence rate per 10,000 full-time workers in construction and extraction occupations was higher for back injuries than for injuries of any upper extremity (arm, shoulder, hand, wrist, and finger) or lower extremity (knee, ankle, foot, toe).15 Each day, construction workers lift materials repeatedly, lift and twist at the same time, bend over for long periods of time, perform sudden movements, and are exposed to whole-body vibration—all these are common causes of back injuries and illnesses.14 Figure 2 illustrates the rate of back injuries and illnesses per 10,000 full-time workers in selected construction occupations in 2005.
Ergonomic risk factors are present in all construction trades, but increased risk of specific MSDs is associated with certain occupations.14,53-58 Figure 2 indicates that laborers are at the greatest risk of back injuries and illnesses.14 The Chartbook of the CPWR (The Center for Construction Research and Training, formerly the Center to Protect Workers’ Rights) points out that laborers are also at the greatest risk for overexertion injuries.14
Hartmann documented that scaffolders, bricklayers, and carpenters regularly handle heavy weights, with resulting excessive pressure on the back.59 And bricklaying required bent postures during as much as 35 percent of daily worktime. Painters, plumbers, and carpenters worked frequently in kneeling postures. In addition, painters often worked with their arms overhead.59 Overhead drilling into concrete or metal is one of the most physically demanding tasks: the work is done with heavy, rotary impact hammer drills.60 Workers who drill into concrete or metal ceilings suffer pain and MSDs at the wrist, forearm, shoulder, and back due to high forces and non-neutral shoulder and wrist postures.60,61

Personal protective equipment should not be the only solution for protecting construction workers’ safety
and health.
How much do construction injuries cost?
In 2009, the construction industry constituted about 4 percent of the total gross domestic product in the United States. The proportion declined steadily from 2006 to 2009 with the slowdown of residential and building construction.62 Various researchers have attempted to estimate how much construction injuries cost.63,64-67 For example, the 2008 Chartbook from CPWR provides a useful summary of costs of work-related injuries and illnesses in the construction sector.14 Calculating an accurate cost estimate for injuries and illnesses is difficult. While certain aspects can be calculated rather easily (e.g., wage replacement, workers’ compensation costs, medical payments, or production losses), other aspects (e.g., the victim’s and family’s suffering) are very hard to capture in numbers.14 Many costs are not compensated, partly because they are difficult to link to specific work exposures. Construction workers may serve several employers —even within a single year—and perhaps have dozens of employers over their careers.14 In addition, occupational illnesses (e.g., noise-induced hearing loss, cancers, neurological disorders) are usually identified long after the start of the exposure and thus may not be successfully linked to a work-related exposure and then compensated. MSDs can be classified either as illnesses due to repeated trauma (e.g., carpal tunnel syndrome and tendinitis) or as injuries due to sprains and strains (e.g., back injuries).14,53 Finally, about one-fourth of the construction workforce is self-employed, and most of these self-employed workers are not covered by workers’ compensation, so that workers’ compensation costs are not captured.63
CPWR estimated the total cost of fatal and nonfatal injuries in the construction industry at nearly $13 billion annually.14,c This is intended to capture direct costs (medical payments), indirect costs (wage losses, household production losses, costs of administering workers’ compensation), as well as quality-of-life costs (pain and suffering of victims and their families). Deaths are estimated to represent 40 percent of the total cost, and nonfatal injuries and illnesses the rest.14 The death of a construction worker is estimated to cost $4 million in losses; a nonfatal injury costs approximately $42,000.14
Waehrer and colleagues developed a cost model based on fatal and non-fatal injuries in the construction industry, its subsectors, and 50 construction occupations, seeking to capture qualityof- life costs along with direct and indirect costs.64,65 The total cost of fatal and nonfatal injuries was estimated at $11.5 billion, representing 15 percent of all injury costs for private industry.64 The average cost per case of fatal or nonfatal injury was estimated at $27,000 in 2002, significantly higher than the cost per case of $15,000 for all industries in 2002.64
Construction laborers and carpenters ranked the highest in costs for both fatal and nonfatal injuries. They account for 40 percent of all the construction industry costs.65 The costs of fatal injuries for construction laborers and carpenters were more than $1.2 billion and $376 million, respectively. The costs of nonfatal injuries to construction laborers amounted to almost $2.1 billion, and to carpenters, about $1.6 billion.65
Horowitz and McCall examined all accepted workers’ compensation claims by Oregon construction employees (N = 20,680) during the period 1990-2007.66 Over 50 percent of claims were filed by workers under 35 years old and with less than one year on the job. The average claim cost was $10,084 and the mean time period (i.e., mean indemnity time) for which a worker received the compensation was 57.3 days.66 Structural metal workers had the highest average days of indemnity (72.1), the highest average costs per claim ($16,472), and the highest injury share of all construction trades examined.66
Immigrant construction workers and the nature of their work
The US construction sector is characterized by a multi-ethnic workforce. In 2008, almost 25 percent of construction workers were foreign born.68 In 2007, more than four-fifths of foreign-born workers originated from either Mexico (59 percent) or another Latin American country (25 percent).68
The share of workers who are Hispanic is greater than 40 percent in drywall installation, roofing, and concrete work, and among laborers (Figure 3). The total number of Hispanic construction workers increased rapidly from 705,000 in 1990 to nearly 3 million in 2007, but dropped sharply during 2007-2008 due to the economic downturn.14
In 2008, 11 percent of Hispanic workers in the construction trades belonged to a union, compared to 18 percent of non-Hispanic workers. Hispanic union members made $7.60 more per hour than their non-union counterparts; however, Hispanic construction workers continue to make less than their white non-Hispanic counterparts, in both union and non-union jobs. Also, the highest paid construction trades have fewer Hispanic workers.
Evidence indicates that Hispanic construction workers are more likely to suffer fatal and non-fatal injuries than their white non-Hispanic co-workers. 69,70 During 1992-2006, fatal falls accounted for nearly 40 percent of all deaths of Hispanic construction workers, compared to 31 percent for white non-Hispanics.13,68,71 Furthermore, Dong and colleagues showed that Hispanic workers were 53 percent more likely to have medical conditions resulting from work-related injuries than their white non-Hispanic counterparts, but 48 percent less likely to receive payment for medical costs from workers’ compensation.63 The average medical cost per injury was about $210 more (12.4 percent higher) for Hispanic construction workers than for white non-Hispanic workers.63
Figure 3:
Percent of workers who are Hispanic in selected trades in 2007.
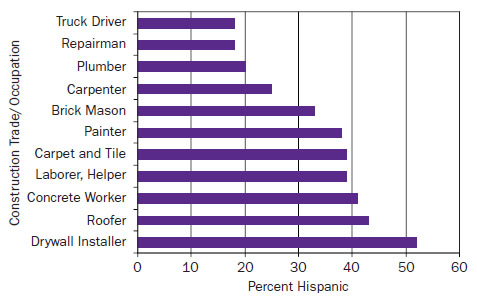
Source: CPWR—The Center for Construction Research and Training.
The Construction Chart Book. 2008. Chart 41d, p41.
New immigrant workers—in particular undocumented workers—experience communication, legal, and cultural barriers to understanding and exercising their workplace rights.63 Many undocumented immigrant workers are day laborers hired from street corners. They are often employed in dangerous conditions and afraid to speak up for their rights for fear of possible retaliation.72,73 Undocumented day laborers have few job alternatives because of their lack of work authorization, weak English, relative youth, limited formal education, and lack of job experience.72 The majority are hired by non-union residential construction contractors or directly by landlords/homeowners to carry out tasks such as roofing (e.g., carrying shingles up to the roof), demolition, drywall installation, painting, and repairs carried out on ladders or scaffolds.72 These employers have typically little awareness of occupational safety and health concerns and rarely use measures to prevent injuries and illnesses (e.g., guard rails and other fall prevention systems, training, personal protective equipment).72
Government action
Since the passage of the OSHAct, OSHA has developed and adopted a number of standards for the construction sector. Most recently, in 2010 OSHA issued the Final Rule on Cranes and Derricks in Construction and also proposed a rule on Walking-Working Surfaces and Personal Protective Equipment (Fall Protection Systems) to prevent injuries from slips, trips and falls.74,75 Furthermore, OSHA has suggested changes in the OSHAct’s General Duty Clause that would extend an employer’s general duty to protect employees from recognized hazards beyond protecting its own employees to protecting contract employees as well.76 These and other key events in the history of occupational safety and health in the construction industry are listed in the timeline that appears at the end of this case study.
Tackling enforcement challenges:
OSHA’s focused inspections
Currently, OSHA has about 1,100 federal inspectors and a considerable amount of their time is devoted to monitoring safety and health conditions in the construction sector.77 The number of construction inspections dropped in the mid- 1990s and has been increasing slightly since 1997. However, the total number of inspections performed in 2006 is about 26 percent lower than in 1988.14 At the same time, the number of construction establishments increased about 47 percent from 1987 to 2005.14 Further, the dynamic nature of construction work creates enforcement challenges that are different from those in a fixed manufacturing location.4
Since 1994, OSHA has been carrying out a “focused” inspection program in the construction industry—looking only at the four leading hazards (falls, struck-by, caught-in-between, and electrocutions). 11 To qualify for a focused inspection, a contractor must have established an effective safety and health program.11 In 2006, 6 percent of OSHA construction inspections were classified as “focused.”14 The focused inspection approach enables inspectors to target their efforts on sites that are likely to be more hazardous. They are thus able to conduct more comprehensive inspections at these sites.
Unions play an important role in safety and health training, information, advocacy, and
support for immigrant construction workers.
National safety and health priorities in the US construction industry
Through the National Occupational Research Agenda of the National Institute for Occupational Safety and Health (NIOSH),10 various stakeholders in the construction sector have developed the National Construction Agenda. The Agenda consists of 15 occupational safety and health priorities to guide the research community and industry in addressing recognized challenges (Table 1).1
Resources are needed not only for the 15 priorities on the National Construction Agenda, but also for recently designated emerging issues relevant to construction workers’ safety and health. Gillen & Gittleman have reviewed and highlighted the following emerging issues:78
- climate change and energy considerations, including not only green construction developments and opportunities but also work-related heat hazards among construction workers (e.g., heat stress/stroke, air pollution, vector-borne diseases, and extreme weather events).
- potential hazards from the use of new materials, in particular nanomaterials or lightweight composites. One such example is titanium dioxide nanoparticles, which are added to cement to break down organic pollutants via catalytic reactions—this allows concrete to retain its whiteness and resist staining. Also, nanoscale silica is added to cement to improve particle packing, increasing the cement density structure, improving the mechanical properties of the cement.
- changes in industry structure and practice to address safety more efficiently. The construction industry’s highly complex structure includes multiple layers of organizations and disciplines simultaneously performing specialized tasks. The communication challenges and selfinterests of these multiple entities can adversely affect both safety planning and safety program implementation, as well as business innovation in general. More integrated delivery of construction and expanded early engagement of all project stakeholders are needed. For example, the architecture community is developing new “integrated practice” approaches to address these limitations and inefficiencies.
- changes in the makeup of the workforce, including the greater presence of immigrant workers and the aging of the workforce.
- underreporting of injuries as well as shifting costs and other burdens from the employer to workers’ families, health insurance, social services, and future employers.
- understanding the root causes of illnesses and injuries, and in particular understanding the connections among the causal factors and processes involved in incidents.
Table 1: Fifteen priorities reflected in strategic goals set by the National Construction Agenda to improve construction workers’ safety and health10
| Reduce traumatic injury/events |
|
| Reduce other health hazards and their impacts |
|
| Address contributing factors |
|
Lessons Learned
Four key strategies emerge from our analysis of construction safety and health: (1) implementing management systems in construction safety and health; (2) implementing construction hazards prevention through design (CHPtD); (3) enhancing training and other supports for immigrant construction workers; and (4) engaging the media to raise awareness and improve safety and health in construction.
Need for an occupational safety and health management systems approach
A complex, very hazardous, dynamic, and fast-paced industry needs a comprehensive and systematic OSH solution. One of the best such approaches is an occupational safety and health management system (OSH-MS). An OSH-MS encompasses every critical function through the plan–do–check–act cycle: workplace policy planning and set-up, implementation and operation of the system, evaluation of the system, and continual improvement of OSH performance. OSHA qualifies for focused inspections those construction contractors that have a comprehensive OSH program (i.e., an OSH-MS) in place at their sites.
Without an OSH-MS, many companies (and not only in the construction field) approach safety and health sporadically. Some corrective action might be taken when serious incidents occur, but these actions rarely tackle root causes or aim toward continual improvement. All too often, incident reporting and tracking are not taken seriously. It is tempting to cut corners when facing deadlines. Even when programs are established at worksites, their goal often seems to be compliance with a certain standard rather than preventing and minimizing as many hazards as possible.79
Management systems have been gaining in popularity ever since the International Organization for Standardization (ISO) passed its Quality Management 9000 Series (in 1986) and its Environmental Management 14000 Series (in 1996).80 OSH was seen as a logical component of both these ISO standards.80 Since then, various frameworks have been developed worldwide, including the International Guidelines for Occupational Safety and Health Management Systems under the leadership of the International Labour Organization (ILO) in 2001 (Figure 4).81 In 1988, the ILO adopted its Safety and Health in Construction Convention (No.167), which has been ratified by 24 countries to date.82,d
In the United States, OSHA proposed a safety and health program rule in 1998 but it was withdrawn in 2002.83 In 2005, the American National Standards Institute (AN SI) adopted an OSH-MS consensus standard. 79 The AN SI OSH-MS standard was developed by a committee of more than 40 OSH specialists representing industry, labor, government, and others.79 The committee was known as the Z10 committee, and hence the standard is generally known as AN SI Z10. To date, many companies have successfully implemented construction safety and health management systems (see sidebar, A success story).
Figure 4: Main elements of the OSH management system of the International Labour Organization

Source: International Labour Organization. Guidelines on
Occupational Safety and Health Management Systems
(ILO-OSH 2001). Figure 2, p5.
Sustaining the Construction Hazard Prevention through Design (CHPtD) movement
Seven recommendations to sustain CHPtD in the United States87
|
In 2007, NIOSH established a national initiative called Prevention through Design (PtD).85 In all business decisions, the PtD approach emphasizes the importance of designing out, or at least minimizing, occupational hazards early in the design stage to prevent occupational injuries and illnesses. The first step for the PtD launch was the 2007 National Workshop, at which stakeholders from eight sectors—including construction—convened to formulate the PtD strategy.85 Construction Hazard Prevention through Design (CHPtD) is a procedure in which construction engineers and architects consider the safety of construction workers as they design a facility.86
| Construction Hazard Prevention through Design (CHPtD) is a procedure in which construction engineers and architects consider the safety of construction workers as they design a facility. |
CHPtD has been recognized and implemented internationally as a feasible method to reduce occupational hazards in construction—in particular in the United Kingdom (UK) and Australia.87 In 1995, the UK passed a law requiring architects and construction engineers to incorporate CHPtD when designing facilities.86 In contrast, in the United States, many professional organizations were not aware of the NIOSH PtD initiative in 2007.
A success story: One corporation’s construction safety and health management system84 As a result of a partnership between AMEC Construction Management, Inc., and OSHA—a partnership that originated in Calumet City, Illinois—comprehensive safety and health management systems have been developed and implemented at participating AMEC job sites. The management systems include these core elements: (1) management leadership and employee involvement; (2) worksite analysis; (3) hazard prevention and control; and (4) safety and health training. For example, the following activities have been undertaken at the sites:
To date, over 2,000 employees have received training through the toolbox talks and new employee orientations. Since the partnership began in April 2002, the overall rate of recordable case incidents for participating AMEC subcontractors declined from 9.1 in 2002 to 2.8 in 2004, a 69 percent reduction. AMEC’s 2004 case incident rate of 2.8 is 59 percent below the 2002 non-residential construction industry national average of 6.9 case incidents. |
In all countries, there seem to be similar challenges in implementing CHPtD, such as designers’ lack of safety expertise and additional costs,86 but in the United States there are some distinct concerns in moving the CHPtD effort further. The most important of these is US architects’ and engineers’ fear of liability for not following standard practices. In contrast, in the United Kingdom and Australia, liability is less of a concern because of legislative requirements for safety. The construction sector stakeholders in the National Workshop developed seven recommendations to sustain CHPtD in the United States (see sidebar).87
Research has identified three distinct benefits of CHPtD: (1) Project decisions that dramatically influence project safety occur early in the project, and are usually made by designers and owners. (2) Since many construction hazards are associated with forces, stresses, dynamic motion, and electricity, it would clearly be beneficial to include site safety in design decisions (e.g., regarding soil cave-ins, the safety of cranes, and protection from falls). (3) Engaging all parties in worker safety is important for both symbolic reasons and for making better plans.86
Emerging issues in the National Construction Agenda (listed above) are particularly relevant to CHPtD.78 There are recommendations to incorporate CHPtD in the US Green Building Council’s (USGBC’s) Leadership in Energy and Environmental Design (LEED) movement.87 The LEED structure has faced criticism for not addressing the safety of construction workers. It is vital that green building and sustainability practices— such as LEED—incorporate prevention of injuries, illnesses, and fatalities during construction.78,87
Hispanics Work Safe Project91 Hispanics Work Safe materials include linguistically and culturally appropriate training modules on construction safety and health, each with three basic components: (1) a description of the most dangerous tasks; (2) identification of the hazards associated with these hazardous tasks; and (3) recommended methods of controlling and reducing the identified hazards. An important training component is an introductory 30-minute lecture (“Welcome, Hispanic Worker!”), which focuses on the following topics: Why is this training important? What are we going to learn? How can we take advantage of the training and translate the knowledge acquired into our own daily work practices? All participants receive a training manual and a set of educational materials. Upon successful completion of the 10-hour course, the participants receive an OSHA 10- hour card, a document that is mandatory for employment in construction in a number of states, including Massachusetts. |
For example, the use of skylights is increasing—and as a green construction and energy conservation measure, this is a good thing. However, falls through fragile skylights have resulted in death or serious injury to construction workers. Design solutions that protect against the risk of falls through skylights during construction, maintenance, and demolition activities include the following:88
- use of non-fragile skylights that withstand the live load associated with a construction or maintenance worker inadvertently stepping on or falling on a skylight;
- installation of a permanent guard or screen over each skylight to handle heavy loads;
- installation of temporary guardrails around the perimeter of a skylight installation area; and
- upgrading of fragile existing skylights by installing permanent guards or screens (the latter are recommended for plastic dome skylights and light-transmitting panels because they can degrade over time).
OSH training, advocacy, and community support to protect immigrant construction workers
The construction sector employs a particularly vulnerable population of immigrant workers. Immigrant workers need proper safety equipment, safe tools and materials, and training in a language they understand. Further, it is essential that immigrant workers neither fear to report nor hesitate to report concerns about workplace OSH problems to OSHA.89
The significance of training cannot be over emphasized, and there is evidence that proper training reduces work injuries. A study by Sokas and colleagues found significant improvements in OSH knowledge and attitudes, as well as improvements in practices on the job, three months after a 10-hour OSH awareness class among both US-born and Mexican-born union construction workers.90 Another study, by Williams and colleagues, showed that participatory training emphasizing active problem solving not only encourages workers to protect themselves but also equips workers with the knowledge they need to make informed decisions on work assignments and work practices.72 Despite economic barriers, limited formal education, undocumented status, and limited control over their work environment, Hispanic day laborers are receptive to OSH training and to protecting themselves and co-workers on the job.72 In addition to training, community support remains crucial for offering a public voice for immigrant labor. Researchers at the University of Massachusetts Lowell have developed educational and training materials especially for Hispanic workers, including materials for the OSHA 10-hour construction training program (see sidebar, Hispanics Work Safe Project).
The media’s role in improving safety
Schneider and Check have analyzed the vital role of the media in preventing construction-related injuries. Changes in legislation, regulations, other policies, and work practices can all be promoted through the media, with a positive effect on construction workers’ lives.92 There are two major challenges in current media reporting: (1) The news media tend to cover catastrophic incidents (e.g., involving cranes) in which several workers die at once, whereas individual fatalities rarely receive coverage. (2) There is no in-depth focus on the “why and how” of the incident. Instead, the media often portray construction injuries and fatalities as unpreventable tragedies.92 These authors emphasized that these challenges present an opportunity for safety and health professionals to: (1) encourage news media to provide deeper, more sustained coverage of construction injuries; and (2) provide data, insights, and expertise that will help reporters and editors to do so. Schneider and Check have provided examples of extraordinary in-depth media reporting of construction-related injuries—for example, Alexandra Berzon’s coverage in the Las Vegas Sun of 11 fatalities among construction workers within 17 months on Las Vegas’ gigantic CityCenter and Cosmopolitan construction projects.93 Berzon’s coverage revealed the patterns, root causes, and potential solutions of the safety problems that led to these fatalities.92 Furthermore, it raised awareness of construction safety among the public and policymakers, resulting in changes across the entire Las Vegas construction industry.92
Final thoughts
This case study has provided an overview of the highly hazardous construction sector and recommended an occupational safety and health management system (OSHMS) approach as the most important key to improving safety in construction. Issuing a national OSH-MS framework for the construction sector should not be an impossible task. In fact, models already exist, including OSHA’s Draft Proposed Safety and Health Program Rule of 1998, ILO-OSH 2001, and AN SI Z10.
It is also vital to keep the momentum going on Construction Hazard Prevention through Design (CHPtD). The stakeholders who participated in the National PtD Workshop felt strongly that a government regulation on CHPtD is not a viable short-term strategy—but that it is important for governmental agencies to continue leading the CHPtD movement. CHPtD is also an avenue to incorporate construction workers’ safety and health in green building and other sustainability programs.
| The media often portray construction injuries and fatalities as unpreventable tragedies. |
It is critical to identify ways to reduce the growing number of fatal and non-fatal injuries among immigrant workers, in particular among day laborers. Workplace training and community support are among the most important interventions. OSH interventions grounded in partnerships with community-based organizations can offer successful strategies for reaching out to immigrant workers, understanding their needs, and developing solutions based on those needs.
The potential exists to improve construction workers’ safety and health by highlighting fundamental issues through in-depth reporting by the traditional media, as well as through internet-based and social media. To enable reporters and editors to provide deeper, more sustained coverage of OSH matters in construction—with adequate data, insights, and expertise—the construction OSH community must develop relationships with media outlets. As a result of this kind of networking, the news media will become less likely to cover only catastrophic incidents or leave the false impression that construction injuries are unpreventable tragedies.
NIOSH-FACE Program recommendations for employers to prevent collisions1
|
We started this case study by describing a struck-by fatality, documented by NIOSH-FACE Program.1 How can occurrences similar to this collision fatality be prevented? The NIOSH investigators developed four recommendations for employers to prevent similar incidents (see sidebar).1,e
In addition to the four recommendations for employers, the NIOSH investigators recommended a specific Prevention-through-Design (PtD) action for manufacturers of equipment (e.g., bulldozers): “manufacturers of heavy equipment should explore the possibility of incorporating collision avoidance technology in their equipment.”1 Radio frequency identification (RFID) tags and tag readers are one such collision warning technology: each worker on foot wears a small RFID tag, each piece of mobile equipment is equipped with a tag reader, and the equipment operator receives a warning when a tag is sensed.1,94

Falls are the most frequent cause of fatal injuries among construction workers in the United States.
OSHA and NIOSH are part of the Roadway Work Zone Safety and Health Alliance, which includes these six other partners from the employers’ and employees’ organizations: American Road and Transportation Builders Association (ARTBA), Associated General Contractors of America (AGC), International Union of Operating Engineers (IUOE), Laborers’ International Union of North America (LIUNA ), LIUNA Education and Training Fund, and National Asphalt Pavement Association (NAPA).95 The Alliance provides construction industry employers, workers (including Spanish-speaking and other high-risk or hard-to-reach workers), and others with information, guidance, and training resources specifically to reduce and prevent exposures to roadway work zone safety and health hazards (e.g. flagger safety, safer deployment of traffic control and direction devices, safer night work precautions, work zone speeding control as well as runover/ backover control).95 The National Work Zone Safety Information Clearinghouse is located at http://www.workzonesafety.org—many tools and documents developed by the Alliance are at this site.
An important overall strategy to prevent collisions in worksites is an Internal Traffic Control Plan to design worksite traffic patterns in such a way that the amount of vehicle backing is reduced and the exposure of workers on foot to vehicles is minimized.96 Collisions happen in part because of limited visibility around the equipment.97 NIOSH has developed blind zone analysis diagrams for various types of construction equipment.97
Case Study 4 - Timeline
| Year | Event |
| 1971 | The first OSHA standards are published in the Federal Register on May 29, 1971, including those for construction. Safety and health standards for the construction industry are found in “Part 1926” under Title 29 of the Code of Federal Regulations (CFR).98 |
| 1973 | The Advisory Committee on Construction Safety and Health (ACCSH) is established to advise OSHA on setting construction standards and policy matters.99 |
| 1978 | At the construction site for a power plant in Willow Island, West Virginia, scaffolding around the cooling tower collapses, killing 51 workers.98 |
| 1978 | In Bridgeport, Connecticut, the collapse of the L’Ambiance Plaza building, under construction, kills 28 workers.98 |
| 1982 | OSHA formally announces the Voluntary Protection Program (VPP) to recognize workplaces with exemplary safety and health management systems and designates the first VPP site.100 |
| 1986 | The International Standardization Organization adopts its Quality Management 9000 Series.81 |
| 1988 | The International Labour Organization (ILO) adopts its Safety and Health in Construction Convention (No. 167, 1988).82 |
| 1989 | OSHA issues its voluntary guidelines for safety and health program management.101 |
| 1990s | Several major construction safety and health standards are finalized.98 |
| 1994 | OSHA begins its focused inspection initiative for contractors who have established and fully implemented a corporate safety and health program and site-specific plans.11 |
| 1996 | The International Standardization Organization adopts its Environmental Management 14000 Series.81 |
| 1998 | OSHA proposes its occupational safety and health program rule (29 CFR 1900.1). The rule will be withdrawn in 2002.102 |
| 2001 | The ILO adopts the International Guidelines for Occupational Safety and Health Management Systems, known as ILO-OSH 2001.81 |
| 2001 | The World Trade Center attack results in a massive “worksite,” where intensive rescue efforts in the midst of unprecedented hazards are followed by more than eight months of demolition and cleanup, and eventually by reconstruction.98 |
| 2002 | OSHA launches its Alliance Program, which brings OSHA together with businesses, trade or professional organizations, unions, and educational institutions.98 |
| 2005 | The American National Standards Institute adopts an occupational safety and health management system consensus standard, known as ANSI Z-10.80 |
| 2007 | NIOSH establishes its national initiative, Prevention through Design (PtD) that focuses on designing out or minimizing occupational hazards and risks early in the design of technology.85 |
| 2007 | On August 1, the I-35W Bridge in Minneapolis, Minnesota, collapses, killing 13 people and injuring 98. A construction worker was among those killed.98 |
| 2007-2008 | Eleven construction workers die within 17 months in CityCenter and Cosmopolitan construction projects in Las Vegas.92 |
| 2008-2009 | Construction accounts for the largest number of work-related fatalities and ranks as the fourth highest for non-fatal serious injuries. |
| 2010 | OSHA issues a final rule on updating the standard for cranes and derricks in construction.75 |
Acknowledgments
We wish to acknowledge valuable injury and illness prevention work by various organizations that have improved safety and health among construction workers in the United States. These organizations include the National Institute for Occupational Safety and Health (NIOSH), NIOSH’s Fatality Assessment and Control Evaluation (FACE) program, CPWR: The Center for Construction Research and Training, the Occupational Safety and Health Administration, the National Safety Council, and many others.
The year 2010 marked the 20th anniversary of the Construction Research Program at NIOSH.101 To celebrate the anniversary, the National Safety Council, NIOSH, and the National Construction Center assembled a special issue of the Journal of Safety Research on construction workers’ safety and health.101 Many articles of this special issue have been cited in this case study. In particular, we would like to give a special acknowledgement to CPWR, which has created significant databanks and summaries on OSH in construction that are available on its website (www.cpwr.com). These resources include: the Construction Chart Book14, Hispanic Employment in Construction, the Electronic Library of Construction Occupational Safety and Health (eLCOSH), and Construction Solutions Database.4,68,102,103
We thank Dr. Laura Welch of CPWR for peer reviewing this case study.
References
- Fatality Assessment and Control Evaluation (FACE) Program, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Construction Worker Dies After Being Run Over By a Bulldozer at a Commercial Construction Site - North Carolina (NIOSH In-house FACE Report 2005-11). 2006. A vailable at: http://www.cdc.gov/niosh/face/In-house/full200511.html. Accessed: November 15, 2010.
- Baron S, Welch L, Lipscomb J. Addressing Health and Safety Hazards in Specific Industries: Agriculture, Construction, and Health Care. Construction Workers by Laura S. Welch. In B Levy, D Wegman, S Baron, et al. (Eds.), Occupational and Environmental Health: Recognizing and Preventing Disease and Injury. 5th edition. Philadelphia (PA): Lippincott Williams and Wilkins. 2006. 668-675.
- Weeks JL. Health and Safety Hazards in the Construction Industry. In JM Stellman (ed.), Encyclopaedia of Occupational Health and Safety. Fourth edition. Vol III: 93.2-93.8. Geneva: International Labour Office, 1998.
- Weil D. Making OSHA Inspections More Effective: Alternatives for Improved Inspection Targeting In the Construction Industry. CPWR—Center for Construction Training and Research. 2004. Available at: http://www.elcosh.org/record/document/701/d000663.pdf. Accessed: November 15, 2010.
- Bureau of Labor Statistics, U.S. Department of Labor. Career Guide to Industries, 2010-11 Edition: Construction. 2010. Available at: http://www.bls.gov/oco/cg/cgs003.htm. Accessed: November 15, 2010.
- National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. NIOSH Safety and Health Topic: Construction. 2009. Available at: http://www.cdc.gov/niosh/topics/construction/. Accessed: November 15, 2010.
- Bureau of Labor Statistics, U.S. Department of Labor. Revisions to the 2008 Census of Fatal Occupational Injuries (CFOI) counts. 2010. Available at: http://www.bls.gov/iif/oshwc/cfoi/cfoi_revised08.pdf. Accessed: November 15, 2010.
- Bureau of Labor Statistics, U.S. Department of Labor. National Census for Fatal Occupational Injuries. 2009. Available at: http://www.bls.gov/news.release/pdf/cfoi.pdf. Accessed: November 15, 2010.
- Bureau of Labor Statistics, U.S. Department of Labor. National Census for Fatal Occupational Injuries in 2009 (Preliminary Results). 2010. Available at: http://www.bls.gov/news.release/pdf/cfoi.pdf. Accessed: November 15, 2010.
- NORA Construction Sector Council. National Occupational Research Agenda (NORA) for Occupational Safety and Health Research and Practice in the U.S. Construction Sector 2008; (10/27/08 Revision). Available at: http://www.cdc.gov/niosh/NORA/comment/agendas/construction/pdfs/ConstOct2008.pdf. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. Focused Inspections in Construction. 1996. Available at: http://www.osha.gov/doc/outreachtraining/htmlfiles/focused.html. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. Preventing Fatal Falls in Construction. 2008. Available at: http://www.osha.gov/doc/falls/preventingfalls.html. Accessed: November 15, 2010.
- CPWR—the Center for Construction Research and Training. Highlights 2009: Endings & Beginnings. 2009. Available at: http://www.cpwr.com/sites/default/files/publications/highlights_2009.pdf. Accessed: November 15, 2010.
- CPWR—the Center for Construction Research and Training. Construction Chart Book. 2008. Available at: https://www.cpwr.com/publications/research-findings-articles/construction-chart-book. Accessed: November 26, 2018.
- Bureau of Labor Statistics, U.S. Department of Labor. Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work, 2008. 2009. Available at: http://www.bls.gov/iif/oshwc/osh/case/osnr0033.pdf. Accessed: November 15, 2010.
- Lipscomb HJ, Schoenfisch AL, Shishlov KS. Non-fatal contact injuries among workers in the construction industry treated in U.S. emergency departments, 1998-2005. J Safety Res. 2010;41(3):191-5.
- Lipscomb HJ, Schoenfisch AL, Shishlov KS, et al. Nonfatal tool- or equipment-related injuries treated in US emergency departments among workers in the construction industry, 1998-2005. Am J Ind Med. 2010;53(6):581-7.
- Tjoe Nij E, Heederik D. Risk assessment of silicosis and lung cancer among construction workers exposed to respirable quartz. Scand J Work Environ Health. 2005;31(Suppl 2):49-56.
- Jarvholm B, Silverman D. Lung cancer in heavy equipment operators and truck drivers with diesel exhaust exposure in the construction industry. Occup Environ Med. 2003;60(7):516-20.
- Koskinen K, Pukkala E, Martikainen R, et al. Different measures of asbestos exposure in estimating risk of lung cancer and mesothelioma among construction workers. J Occup Environ Med. 2002;44(12):1190-6.
- Purdue MP, Gold L, Jarvholm B, et al. Impaired lung function and lung cancer incidence in a cohort of Swedish construction workers. Thorax. 2007;62(1):51-6.
- Meeker JD, Cooper MR, Lefkowitz D, et al. Engineering control technologies to reduce occupational silica exposures in masonry cutting and tuckpointing. Public Health Rep. 2009;124 Suppl 1:101-11.
- Akbar-Khanzadeh F, Milz S, Ames A, et al. Crystalline silica dust and respirable particulate matter during indoor concrete grinding—wet grinding and ventilated grinding compared with uncontrolled conventional grinding. J Occup Environ Hyg. 2007;4(10):770-9.
- Meeker JD, Susi P, Pellegrino A. Exposure to silica and metals among painters using specular hematite abrasive. J Occup Environ Hyg. 2005;2(8):D60-4.
- Y asui S, Susi P, McClean M, et al. Assessment of silica exposure and engineering controls during tuckpointing. Appl Occup Environ Hyg. 2003;18(12):977-84.
- Flynn MR, Susi P. Engineering controls for selected silica and dust exposures in the construction industry—a review. Appl Occup Environ Hyg. 2003;18(4):268-77.
- Rappaport SM, Goldberg M, Susi P, et al. Excessive exposure to silica in the US construction industry. Ann Occup Hyg. 2003;47(2):111-22.
- Shepherd S, Woskie SR, Holcroft C, et al. Reducing silica and dust exposures in construction during use of powered concrete-cutting hand tools: efficacy of local exhaust ventilation on hammer drills. J Occup Environ Hyg. 2009;6(1):42-51.
- Woskie SR, Kalil A, Bello D, et al. Exposures to quartz, diesel, dust, and welding fumes during heavy and highway construction. AIHA J (Fairfax, Va). 2002;63(4):447-57.
- Bello D, Virji MA, Kalil AJ, et al. Quantification of respirable, thoracic, and inhalable quartz exposures by FT-IR in personal impactor samples from construction sites. Appl Occup Environ Hyg. 2002;17(8):580-90.
- Virji MA, Bello D, Woskie SR, et al. Analysis of quartz by FT-IR in air samples of construction dust. Appl Occup Environ Hyg. 2002;17(3):165-75.
- Engholm G, Englund A. Asbestos hazard in the Swedish construction industry—recent trends in mesothelioma incidence. Scand J Work Environ Health. 2005;31(Suppl 2):27-30.
- Fonte R, Gambettino S, Melazzini M, et al. Asbestos-induced peritoneal mesothelioma in a construction worker. Environ Health Perspect. 2004;112(5):616-9.
- Merler E, Bressan V, Somigliana A. [Mesothelioma in construction workers: risk estimate, lung content of asbestos fibres, claims for compensation for occupational disease in the Veneto Region mesothelioma register]. Med Lav. 2009;100(2):120-32.
- Welch LS, Haile E. Asbestos-related disease among sheet metal workers 1986-2004: radiographic changes over time. Am J Ind Med. 2009;52(7):519-25.
- Dement JM, Ringen K, Welch LS, et al. Mortality of older construction and craft workers employed at Department of Energy (DOE) nuclear sites. Am J Ind Med. 2009;52(9):671-82.
- Dement JM, Welch L, Ringen K, et al. Airways obstruction among older construction and trade workers at Department of Energy nuclear sites. Am J Ind Med. 2010;53(3):224-40.
- Guo YL, Wang BJ, Yeh KC, et al. Dermatoses in cement workers in southern Taiwan. Contact Dermatitis. 1999;40(1):1-7.
- Chou TC, Chang HY, Chen CJ, et al. Effect of hand dermatitis on the total body burden of chromium after ferrous sulfate application in cement among cement workers. Contact Dermatitis. 2008;59(3):151-6.
- Chen CJ, Shih TS, Chang HY, et al. The total body burden of chromium associated with skin disease and smoking among cement workers. Sci Total Environ. 2008;391(1):76-81.
- Macedo MS, de Avelar Alchorne AO , Costa EB, et al. Contact allergy in male construction workers in Sao Paulo, Brazil, 2000-2005. Contact Dermatitis. 2007;56(4):232-4.
- Uter W, Ruhl R, Pfahlberg A, et al. Contact allergy in construction workers: results of a multifactorial analysis. Ann Occup Hyg. 2004;48(1):21-7.
- Katsarou-Katsari A, Bankovska E, Lambrinopoulou K, et al. Trends in allergic contact dermatitis and preventive measures among cement workers (1985-1999). Contact Dermatitis. 2003;48(3):174-5.
- Bock M, Schmidt A, Bruckner T, et al. Occupational skin disease in the construction industry. Br J Dermatol. 2003;149(6):1165-71.
- Winder C, Carmody M. The dermal toxicity of cement. Toxicol Ind Health. 2002;18(7):321-31.
- Tak S, Roscoe RJ, Alarcon W, et al. Characteristics of US workers whose blood lead levels trigger the medical removal protection provision, and conformity with biological monitoring requirements, 2003-2005. Am J Ind Med. 2008;51(9):691-700.
- Virji MA, Woskie SR, Pepper LD. Task-based lead exposures and work site characteristics of bridge surface preparation and painting contractors. J Occup Environ Hyg. 2009;6(2):99-112.
- Virji MA, Woskie SR, Pepper LD. Skin and surface lead contamination, hygiene programs, and work practices of bridge surface preparation and painting contractors. J Occup Environ Hyg. 2009;6(2):131-42.
- Flynn MR, Susi P. Neurological risks associated with manganese exposure from welding operations—a literature review. Int J Hyg Environ Health. 2009;212(5):459-69.
- Flynn MR, Susi P. Manganese, iron, and total particulate exposures to welders. J Occup Environ Hyg. 2010;7(2):115-26.
- Meeker JD, Susi P, Flynn MR. Manganese and welding fume exposure and control in construction. J Occup Environ Hyg. 2007;4(12):943-51.
- Welch LS, Rappaport SM, Susi P. Construction welding exposures to manganese likely to exceed proposed TLV. J Occup Environ Hyg. 2004;1(6):D63-5.
- Schneider SP. Musculoskeletal injuries in construction: a review of the literature. Appl Occup Environ Hyg. 2001;16(11):1056-64.
- Buchholz B, Paquet V, Wellman H, et al. Quantification of ergonomic hazards for ironworkers performing concrete reinforcement tasks during heavy highway construction. AIHA J (Fairfax, Va). 2003;64(2):243-50.
- Kittusamy NK, Buchholz B. Whole-body vibration and postural stress among operators of construction equipment: a literature review. J Safety Res. 2004;35(3):255-61.
- Moir S, Paquet V, Punnett L, et al. Making sense of highway construction: a taxonomic framework for ergonomic exposure assessment and intervention research. Appl Occup Environ Hyg. 2003;18(4):256-67.
- Paquet V, Punnett L, Woskie S, et al. Reliable exposure assessment strategies for physical ergonomics stressors in construction and other non-routinized work. Ergonomics. 2005;48(9):1200-19.
- Tak S, Paquet V, Woskie S, et al. Variability in risk factors for knee injury in construction. J Occup Environ Hyg. 2009;6(2):113-20.
- Hartmann B, Fleischer, AG. Physical load exposure at construction sites. Scand J Work Environ Health. 2005;31(Suppl 2):88-95.
- Rempel D, Star D, Barr A, et al. Field evaluation of a modified intervention for overhead drilling. J Occup Environ Hyg. 2010;7(4):194-202.
- Rempel D, Star D, Barr A, et al. Overhead drilling: comparing three bases for aligning a drilling jig to vertical. J Safety Res. 2010;41(3):247-51.
- U.S. Bureau of Economic Analysis. Gross-Domestic-Product-by-Industry Accounts: Value Added by Industry as a Percentage of Gross Domestic Product. 2010. Available at: http://www.bea.gov/industry/gpotables/gpo_action.cfm?anon=506501&table_id=25696&format_type=0. Accessed: November 15, 2010.
- Dong X, Ringen K, Men Y, et al. Medical costs and sources of payment for work-related injuries among Hispanic construction workers. J Occup Environ Med. 2007;49(12):1367-75.
- Waehrer GM, Dong XS, Miller T, et al. Costs of occupational injuries in construction in the United States. Accid Anal Prev. 2007;39(6):1258-66.
- Waehrer GM, Dong XS, Miller T, et al. Occupational injury costs and alternative employment in construction trades. J Occup Environ Med. 2007;49(11):1218-27.
- Horwitz IB, McCall BP. Disabling and fatal occupational claim rates, risks, and costs in the Oregon construction industry 1990-1997. J Occup Environ Hyg. 2004;1(10):688-98.
- National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. NIOSH Fatal Occupational Injury Cost Fact Sheet: Construction. 2006. Available at: http://www.cdc.gov/niosh/docs/2006-153/. Accessed: November 15, 2010.
- CPWR - the Center for Construction Research and Training. Hispanic Employment in Construction. 2009. Available at: http://www.cpwr.com/sites/default/files/publications/Hispanic_Data_Brief-Nov-09_1.pdf. Accessed: November 15, 2010.
- Dong X, Platner JW. Occupational fatalities of Hispanic construction workers from 1992 to 2000. Am J Ind Med. 2004;45(1):45-54.
- Dong XS, Men Y, Ringen K. Work-related injuries among Hispanic construction workers-evidence from the medical expenditure panel survey. Am J Ind Med. 2010;53(6):561-9.
- Dong XS, Fujimoto A, Ringen K, et al. Fatal falls among Hispanic construction workers. Accid Anal Prev. 2009;41(5):1047-52.
- Williams Q, Jr., Ochsner M, Marshall E, et al. The impact of a peer-led participatory health and safety training program for Latino day laborers in construction. J Safety Res. 2010;41(3):253-61.
- Solis HS. A preventable epidemic: Latino deaths on the job. The Huston Chronicle. April 20, 2010. Available at: http://www.chron.com/disp/story.mpl/editorial/outlook/6967754.html. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. US Department of Labor’s OSHA publishes final rule on cranes and derricks in construction. 2010. Available at: http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=NEWS_ RELEASES&p_id=18048. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. Occupational Safety and Health Administration. Proposed Rule: Walking-Working Surfaces and Personal Protective Equipment (Fall Protection Systems). Federal Register. May 24, 2010; 75:28862-29153. Available at: http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=FEDERAL_ REGISTER&p_id=21518. Accessed: November 15, 2010.
- Testimony of David Michaels, Assistant Secretary for Occupational Safety and Health, U.S. Department of Labor. The Committee on Health, Education, Labor and Pensions, U.S. Senate. 2010. Available at: http://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table= TESTIMONIES&p_id=1122. Accessed: November 15, 2010.
- Weil D. A strategic approach to labour inspection. International Labour Review. 2008;147(4):349-375.
- Gillen M, Gittleman JL. Path forward: emerging issues and challenges. J Safety Res. 2010;41(3):301-6.
- Palassis J, Schulte PA, Geraci CL. A new American management systems standard in occupational safety and health – ANSI Z10. Journal of Chemical Health & Safety. 2006(January/February):20-23.
- International Labour Organization. About the ILO OSH-MS Guidelines. 2001. Available at: http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_110496.pdf. Accessed: November 15, 2010.
- International Labour Organization. Guidelines on occupational safety and health management systems. (ILO-OSH 2001). 2001. Available at: http://www.ilo.org/public/libdoc/ilo/2001/101B09_287_engl.pdf. Accessed: November 17, 2010.
- International Labour Organization. Safety and Health in Construction Convention. 1988(No. 167). Available at: http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C167. Accessed: November 15, 2010.
- Occupational Safety and Health Administration. Draft Proposed Safety and Health Program Rule: 29 CFR 1900.1, Docket No. S&H-0027. 1998. Available at: http://www.osha.gov/dsg/topics/safetyhealth/nshp.html. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. AMEC Construction Partnership implements safety and health management systems and reduces injury and illness incident rate. 2010. Available at: http://www.osha.gov/dcsp/success_stories/partnerships/region5/191_amec_success.html. Accessed: November 15, 2010.
- National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. Prevention through Design. Available at: http://www.cdc.gov/niosh/topics/ptd/. Accessed: November 15, 2010.
- Toole TM, Gambatese J. The trajectories of Prevention through Design in construction. J Safety Res. 2008;39(2):225-30.
- Behm M. Construction sector. J Safety Res. 2008;39(2):175-8.
- OSHA Alliance Program’s Construction Roundtable. Construction Workplace Design Solution: Non-Fragile Skylights and/or Skylight Guards. 2010. Available at: http://www.designforconstructionsafety.org/media.shtml. Accessed: November 15, 2010.
- Hassan M. OSHA urges Morris County NJ Latino workers to report safety violations. Daily Record. July 27, 2010.
- Sokas RK, Emile J, Nickels L, et al. An intervention effectiveness study of hazard awareness training in the construction building trades. Public Health Rep. 2009;124 Suppl 1:160-8.
- Hispanics Work Safe Project. Training & Educational Materials for Hispanic Construction Workers: OSHA 10-hr Construction Training Course. Available at: http://usfoticenter.org/10-hour-construction/. Accessed: November 15, 2010.
- Schneider S, Check P. Read all about it: the role of the media in improving construction safety and health. J Safety Res. 2010;41(3):283-7.
- Berzon A. Construction Worker Deaths on the Strip: Pace is the new peril. Amid pressure to finish massive projects, 9 men have died in 16 months. Las Vegas Sun. March 30, 2008.Available at: http://www.lasvegassun.com/news/2008/mar/30/construction-deaths/. Accessed: November 15, 2010.
- National Institute for Occupational Safety and Health. Building safer highway work zones: measures to prevent worker injuries from vehicles and equipment. DHHS (NIOSH) Publication No. 2001-128. 2002. Available at: http://www.cdc.gov/niosh/docs/2001-128/. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. OSHA Alliance Program: The Roadway Work Zone Safety and Health Partners. Available at: http://www.osha.gov/dcsp/alliances/roadway/roadway.html. Accessed: November 15, 2010.
- The Roadway Safety Alliance. Internal Traffic Control Plans. 2005. Available at: http://www.workzonesafety.org/files/documents/training/fhwa_wz_grant/itcp.pdf. Accessed: November 15, 2010.
- National Institute for Occupational Safety and Health. Highway Work Zone Safety: Construction Equipment Visibility. 2002. Available at: http://www.cdc.gov/niosh/topics/highwayworkzones/BAD/. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. Reflections on OSHA’s History. 2009. Available at: http://www.osha.gov/history/OSHA_HISTORY_3360s.pdf. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. ACCSH: Background, History, and Charter. Available at: http://www.osha.gov/doc/accsh/backgroundandhist.html. Accessed: November 15, 2010.
- Occupational Safety and Health Administration, U.S. Department of Labor. Voluntary Protection Programs: All About VPP. Available at: http://www.osha.gov/dcsp/vpp/all_about_vpp.html. Accessed: November 15, 2010.
- Howard J, Stafford P, Branche C, et al. Twenty years of NIOSH construction research. J Safety Res. 2010;41(3):187-8.
- CPWR—the Center for Construction Research and Training. Electronic Library for Construction Occupational Safety and Health (eLCOSH). CPWR—the Center for Construction Research and Training. Available at:http://www.elcosh.org/. November 15, 2010.
- CPWR—the Center for Construction Research and Training. Construction Solutions. Database. 2010. Available at: http://www.cpwrConstructionSolutions.org/. Accessed: November 15, 2010.
a Based on the US Bureau of Labor Statistics’ total fatality cases (975) in construction, in 2008.
b Based on the US Bureau of Labor Statistics’ total non-fatal cases (120,240) in construction, in 2008.
c CPWR estimates in this paragraph are all based on the 2002 dollar value.
d The United States has not ratified the ILO’s Safety and Health in Construction Convention (No. 167, 1988). The only ILO Convention related to occupational safety and health that the United States has ratified (in 2001) is the Safety and Health in Mines Convention (No. 176. 1995).
e The NIOSH-FACE report offers more detailed discussion of each recommendation at http://www.cdc.gov/niosh/face/In-house/full200511.html.