
Warehouse Worker Crushed by Forks of Laser Guided Vehicle
-
Fatality Assessment and Control Evaluation (FACE) Program Reports
The National Institute for Occupational Safety and Health’s (NIOSH) Fatality Assessment and Control Evaluation (FACE) Program and State FACE Programs study fatal workplace injuries and prepare reports with recommendations to prevent similar injuries. The following are links to all of the items in this collection:
Documents
- Kentucky FACE Report: Commercial Roofer Falls 30 Feet Through a Skylight While Installing Roof Insulation
- Fatal Occupational Injuries in Massachusetts 2008-2013
- Fatality Assessment & Control Evaluation (FACE) Program
- Washington FACE Report: Glazier Foreman Falls From Stepladder
- Preventing Construction Falls Toolkit
- Hazard Alert: Pedestrian Workers Killed by Forklifts
- Keep Employees in Motor Vehicles Safe
- New York FACE Brochure
- Washington FACE Report: Construction Laborer Falls When Ladder Breaks
- Washington FACE Report: Pipelayer Dies when Trench Wall Collapses
- Washington FACE Report: Carpenter Falls 60 Feet from Bridge Concrete Form
- Washington FACE Report: Foreman and Laborer Fall when Aerial Lift Struck by Vehicle
- Washington FACE Report: Framer Falls 18 Feet while Sheathing Roof
- New York FACE Report: Mechanic Electrocuted when a Mobile Light Tower Contacted Powerline
- New York FACE Report: Two Construction Workers Fatally Crushed when Cement Formwork Collapsed
- Kentucky FACE Report: Construction Laborer Killed in Trench Collapse while Taking Grade Measurements
- California FACE Report: A Heating, Ventilaton and Air Conditioning (HVAC) Contractor Dies when He Falls through a Skylight
- Massachusetts FACE Report: Carpenter Fatally Injured after Falling from an Extension Ladder
- Massachusetts FACE Report: Laborer Fatally Injured after Falling from a Home under Construction
- Oregon FACE Report: Worker Falls When Ladder Slips
- Michigan FACE Information Sheet: Look for Mobile Equipment Blind Spots
- Oregon FACE Report: Collapsed roof trusses kill carpenter foreman
- Washington FACE Report: Roofer Falls 19 Feet from Roof
- Hazard Alert: Plan. Provide. Train. Prevent Fall Injuries & Deaths
- Kentucky FACE Report: 19-Year-Old Construction Laborer Crushed in Trench Collapse While Laying Sewage Pipe
- Kentucky FACE Report: Construction Flagger Struck and Killed in Two-Lane Highway Work Zone
- Kentucky FACE Report:Temporary Electrician Helper Steps into Unguarded Elevator Shaft and Dies
- Fatality Narrative: Roofing Contractor Falls 25 Feet From Church Roof
- Kentucky FACE Report: Construction Siding Subcontractor Installer Killed when Oversized Scaffolding Platform Destabilized and Telescopic Forklift Overturned
- NIOSH FACE Report - Maintenance Worker Struck by Forklift Carriage—Tennessee
- Kentucky Hazard Alert: Roofing and Construction Workers Killed Due to High Winds
- Poster: Secure it to move it!
- Oregon FACE Report: Crane Operator Killed By Falling Steel Beam
- New Jersey FACE Report: Mechanic Dies After Being Crushed Under Electrical Cabinet
- New Jersey FACE Report: Plant Manager Crushed to Death Under Fallen Pile of Steel Beams
- NIOSH FACE Report: Hispanic worker falls from residential roof
- Oregon FACE Report: Construction worker died after falling 20-25 feet from a pump-jack scaffold
- FACE Fact Sheet: Prevent Construction Falls from Roofs, Ladders, and Scaffolds
- Construction Fatality Narrative: Roofer Falls 18 Feet from Wet House Roof
- Construction Worker Killed when Trench Collapsed, Oregon
- A Tree Trimmer is Electrocuted While Trimming a Palm Tree
- A Tree Feller Dies When Struck By a Tree Limb While Felling a Fire-Damaged Tree
- Concrete Finisher Electrocuted When Bull Float Contacted an Energized Power Line
- Warehouse Worker Crushed by Forks of Laser Guided Vehicle
Summary Statement
In December 2015, a 45-year-old warehouse dock coordinator at a water bottling company died after he was crushed when the elevated forks of an automatic laser guided vehicle came down on him.
The company used driverless forklifts, known as laser guided vehicles (LGVs), in the warehouse to move pallets of water bottles. LGVs automatically navigated using a system of vehicle mounted lasers and reflectors positioned throughout the warehouse. Each LGV had safety sensors designed to detect objects or workers in the vehicle’s path. When a sensor detected an obstacle, the LGV would stop moving and an alarm would sound until a worker removed the obstacle.
The manufacturer’s manual required workers to initiate an emergency stop before removing an obstacle detected by the LGV. An LGV would then have to be manually reset before restarting its task. Without initiating an emergency stop, the LGVs would resume automatic function immediately after an obstruction was removed.
The victim was working in the warehouse when an LGV alarm was activated. Shortly after, another worker heard noises over the radio and looked into the warehouse to investigate. He saw the victim slumped over one of the LGVs. The LGV then started moving again, and the other worker hurried to it and initiated an emergency stop. He could see that the victim had severe injuries to his chest and jaw. He called for help and called 911. Emergency responders arrived within minutes and transported the victim to a local hospital where he was pronounced dead.
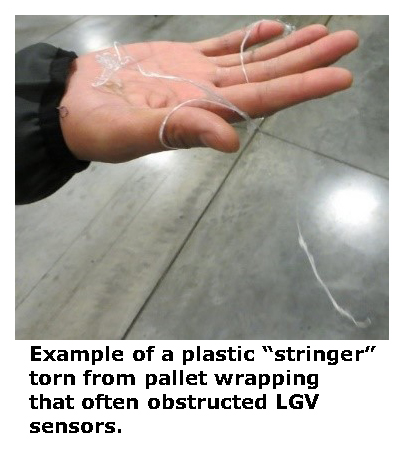
Investigators believe that the victim attempted to remove a piece of plastic from under the elevated forks of the LGV without first initiating an emergency stop. Long strips of plastic wrap often tore off of pallets during loading and unloading and stuck to the forks of the LGVs. If the plastic entered the safety detection field of the LGV, it would be recognized as an obstacle. Other employees said that these plastic “stringers” frequently triggered LGV alarms. The victim was likely bending or kneeling under the forks outside of the safety sensor field to reach the plastic stringer. Because the LGV was not in emergency stop mode, the system reset when the obstacle was removed, bringing the elevated forks down, crushing him against the wheel cover of the vehicle.
There were warning signs affixed to the vehicle indicating that workers should avoid standing beneath the elevated forks.
April 2019
Incident Facts

REPORT #: 71-171-2018
REPORT DATE: 5/10/2018
INCIDENT DATE: 12/9/2015
VICTIM: 45 years old, Employed at facility for approximately one year
INDUSTRY: Bottled water manufacturing
OCCUPATION: Warehouse dock coordinator
SCENE: Water bottling plant warehouse
EVENT TYPE: Crush

Requirements
 Employers must protect workers around PITs (powered industrial trucks), and not allow them under the elevated part of any PIT, whether it is loaded or empty. See WAC 296-863-4005(2)(a).
Employers must protect workers around PITs (powered industrial trucks), and not allow them under the elevated part of any PIT, whether it is loaded or empty. See WAC 296-863-4005(2)(a).
Recommendations
FACE investigators concluded that, to help prevent similar occurrences, employers should:
- Incorporate manufacturer safety requirements into written company safety procedures for automated guided industrial vehicles.
- Train workers about the specific hazards and safety requirements associated with automated guided industrial vehicles, like LGVs. Emphasize that workers are expected to follow required safety procedures every time, and ensure compliance through periodic refresher training and spot checks
For a PDF formatted as a slideshow, click here.
 This narrative is an alert about the tragic loss of life of a worker and is based on preliminary data ONLY and does not represent final determinations regarding the nature of the incident or the cause of the fatality. Developed by WA State Fatality Assessment and Control Evaluation (FACE) Program and the Division of Occupational Safety and Health (DOSH), WA State Dept. of Labor & Industries. The FACE Program is supported in part by a grant from the National Institute for Occupational Safety and Health (NIOSH grant# 5U60OH008487). For more information visit www.lni.wa.gov/Safety/Research/FACE.
This narrative is an alert about the tragic loss of life of a worker and is based on preliminary data ONLY and does not represent final determinations regarding the nature of the incident or the cause of the fatality. Developed by WA State Fatality Assessment and Control Evaluation (FACE) Program and the Division of Occupational Safety and Health (DOSH), WA State Dept. of Labor & Industries. The FACE Program is supported in part by a grant from the National Institute for Occupational Safety and Health (NIOSH grant# 5U60OH008487). For more information visit www.lni.wa.gov/Safety/Research/FACE.